

Reducing diagnostic errors through effective communication: harnessing the power of information technology
- PMID: 18373151
- PMCID: PMC2359508
- DOI: 10.1007/s11606-007-0393-z
Reducing diagnostic errors through effective communication: harnessing the power of information technology
Abstract
Diagnostic errors are poorly understood despite being a frequent cause of medical errors. Recent efforts have aimed to advance the "basic science" of diagnostic error prevention by tracing errors to their most basic origins. Although a refined theory of diagnostic error prevention will take years to formulate, we focus on communication breakdown, a major contributor to diagnostic errors and an increasingly recognized preventable factor in medical mishaps. We describe a comprehensive framework that integrates the potential sources of communication breakdowns within the diagnostic process and identifies vulnerable steps in the diagnostic process where various types of communication breakdowns can precipitate error. We then discuss potential information technology-based interventions that may have efficacy in preventing one or more forms of these breakdowns. These possible intervention strategies include using new technologies to enhance communication between health providers and health systems, improve patient involvement, and facilitate management of information in the medical record.
Figures
 Interpersonal communication,
Interpersonal communication,  Informational communication,
Informational communication,  Interpersonal communication,
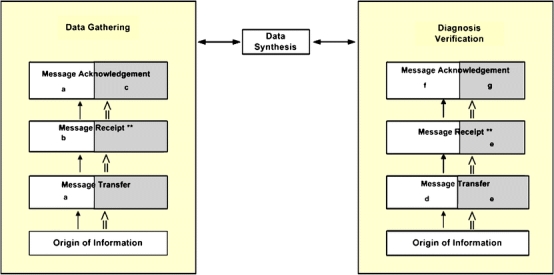
Interpersonal communication,  Informational communication. a. Collaborative goal-setting using an Information Technology platform (Example 1 from table), b. Use of personal health records (Example 2), c. Using electronic progress notes requiring co-signatures of physician (Example 5), d. Electronic Medical Record generated report transmitted to pager or mobile phone of referring physician (Example 7), e. Use of alerts for abnormal test results (Example 10), f. Electronic Medical Record generated reminders to patient and physician (Example 3), g. Using software to track unacknowledged alerts (Example 12)
Informational communication. a. Collaborative goal-setting using an Information Technology platform (Example 1 from table), b. Use of personal health records (Example 2), c. Using electronic progress notes requiring co-signatures of physician (Example 5), d. Electronic Medical Record generated report transmitted to pager or mobile phone of referring physician (Example 7), e. Use of alerts for abnormal test results (Example 10), f. Electronic Medical Record generated reminders to patient and physician (Example 3), g. Using software to track unacknowledged alerts (Example 12)References
-
- Chandra A, Nundy S, Seabury SA. The growth of physician medical malpractice payments: evidence from the National Practitioner Data Bank. Health Aff (Millwood). 2005;Suppl Web Exclusives:W5. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1136/qshc.2003.008029', 'is_inner': False, 'url': 'https://doi.org/10.1136/qshc.2003.008029'}, {'type': 'PMC', 'value': 'PMC1743812', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC1743812/'}, {'type': 'PubMed', 'value': '15069219', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15069219/'}]}
- Phillips RL Jr, Bartholomew LA, Dovey SM, Fryer GE Jr, Miyoshi TJ, Green LA. Learning from malpractice claims about negligent, adverse events in primary care in the United States. Qual Saf Health Care. 2004;13:121–6. - PMC - PubMed
-
- None
- Golodner L. How the public perceives patient safety. Newsletter of the National Safety Foundation. 2004;1997:1–6.
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1001/archinte.167.3.302', 'is_inner': False, 'url': 'https://doi.org/10.1001/archinte.167.3.302'}, {'type': 'PubMed', 'value': '17296888', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/17296888/'}]}
- Singh H, Thomas EJ, Khan M, Petersen LA. Identifying diagnostic errors in primary care using an electronic screening algorithm. Arch Intern Med. 2007;167(3):302–8. - PubMed
-
- Singh H, Thomas EJ, Petersen LA, Studdert DM. Medical errors involving trainees: a study of closed malpractice claims from 5 insurers. Arch Intern Med. 2007 Oct 22;167(19):2030–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
