

Impact of resting heart rate on outcomes in hypertensive patients with coronary artery disease: findings from the INternational VErapamil-SR/trandolapril STudy (INVEST)
- PMID: 18375982
- PMCID: PMC2805436
- DOI: 10.1093/eurheartj/ehn123
Impact of resting heart rate on outcomes in hypertensive patients with coronary artery disease: findings from the INternational VErapamil-SR/trandolapril STudy (INVEST)
Abstract
Aim: To determine the relationship between resting heart rate (RHR) and adverse outcomes in coronary artery disease (CAD) patients treated for hypertension with different RHR-lowering strategies.
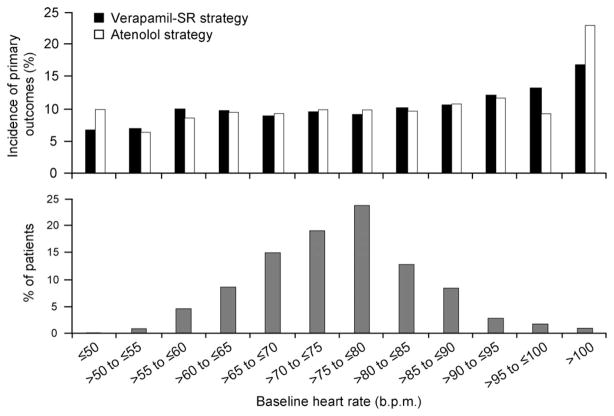
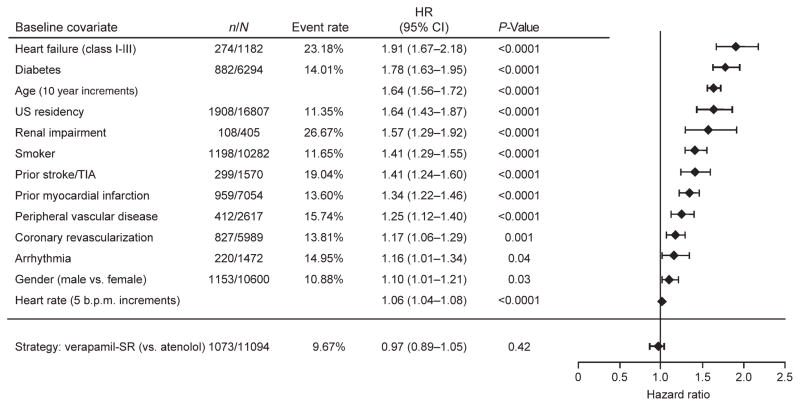
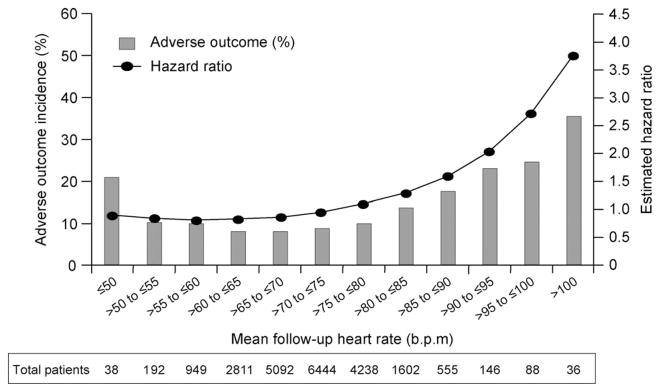
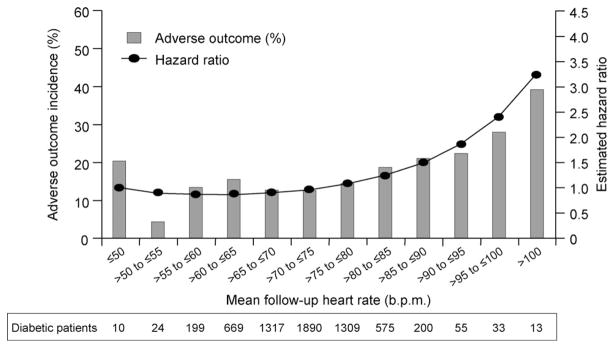
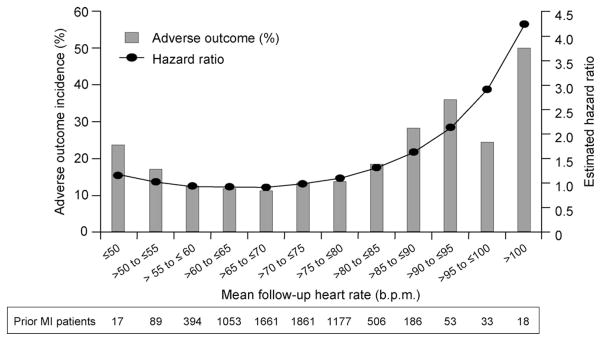
Methods and results: Time to adverse outcomes (death, non-fatal myocardial infarction, or non-fatal-stroke) and predictive values of baseline and follow-up RHR were assessed in INternational VErapamil-SR/trandolapril STudy (INVEST) patients randomized to either a verapamil-SR (Ve) or atenolol (At)-based strategy. Higher baseline and follow-up RHR were associated with increased adverse outcome risks, with a linear relationship for baseline RHR and J-shaped relationship for follow-up RHR. Although follow-up RHR was independently associated with adverse outcomes, it added less excess risk than baseline conditions such as heart failure and diabetes. The At strategy reduced RHR more than Ve (at 24 months, 69.2 vs. 72.8 beats/min; P < 0.001), yet adverse outcomes were similar [Ve 9.67% (rate 35/1000 patient-years) vs. At 9.88% (rate 36/1000 patient-years, confidence interval 0.90-1.06, P = 0.62)]. For the same RHR, men had a higher risk than women.
Conclusion: Among CAD patients with hypertension, RHR predicts adverse outcomes, and on-treatment RHR is more predictive than baseline RHR. A Ve strategy is less effective than an At strategy for lowering RHR but has a similar effect on adverse outcomes.
Conflict of interest statement
Figures
Comment in
-
Is there benefit of cardiac slowing drugs in the treatment of hypertensive patients with elevated heart rate?Eur Heart J. 2008 May;29(10):1218-20. doi: 10.1093/eurheartj/ehn164. Epub 2008 Apr 15. Eur Heart J. 2008. PMID: 18413306 No abstract available.
-
High resting heart rate: a cardiovascular risk factor or a marker of risk?Eur Heart J. 2008 Nov;29(22):2823-4. doi: 10.1093/eurheartj/ehn447. Epub 2008 Oct 1. Eur Heart J. 2008. PMID: 18829611 No abstract available.
References
-
- Cook S, Togni M, Schaub MC, Wenaweser P, Hess OM. High heart rate: a cardiovascular risk factor? Eur Heart J. 2006;27:2387–2393. - PubMed
-
- Levine HJ. Rest heart rate and life expectancy. J Am Coll Cardiol. 1997;30:1104–1106. - PubMed
-
- Stamler J, Berkson DM, Dyer A, Lepper MH, Lindberg HA, Paul O, McKean H, Rhomberg P, Schoenberger JA, Shekelle RB, Stamler R. Relationship of multiple variables to blood pressure—findings from four Chicago epidemiologic studies. In: OP, editor. Epidemiology and Control of Hypertension. Symposia Specialists; Miami: 1975. pp. 307–352.
-
- Eriksson J, Rodahl K. Resting heart rate in apparently healthy middle-aged men. Eur J Appl Physiol. 1979;42:61–69. - PubMed
-
- Berenson GS, Voors AW, Webber LS, Dalferes ER, Jr, Harsha DW. Racial differences of parameters associated with blood pressure levels in children—the Bogalusa Heart Study. Metabolism. 1979;28:1218–1228. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
