

CCL3L1-CCR5 genotype influences durability of immune recovery during antiretroviral therapy of HIV-1-infected individuals
- PMID: 18376407
- PMCID: PMC2630879
- DOI: 10.1038/nm1741
CCL3L1-CCR5 genotype influences durability of immune recovery during antiretroviral therapy of HIV-1-infected individuals
Abstract
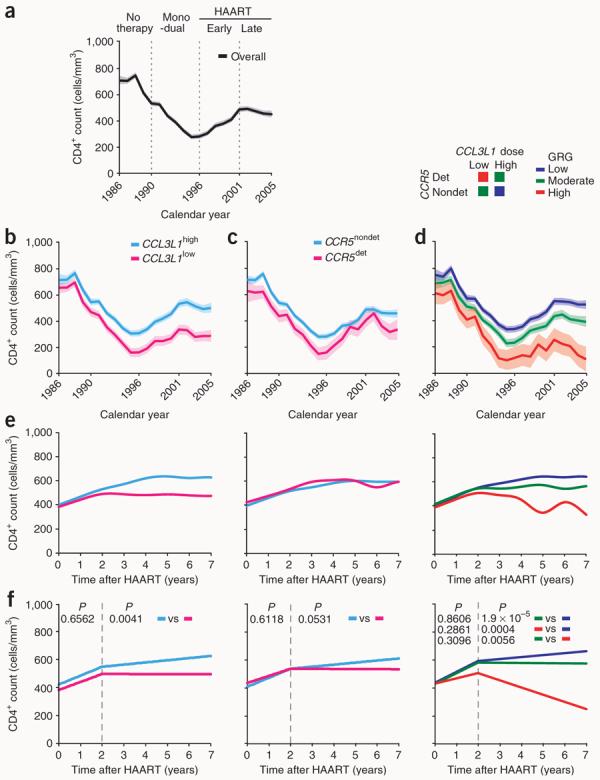
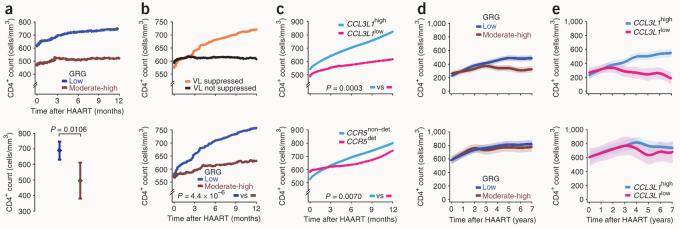
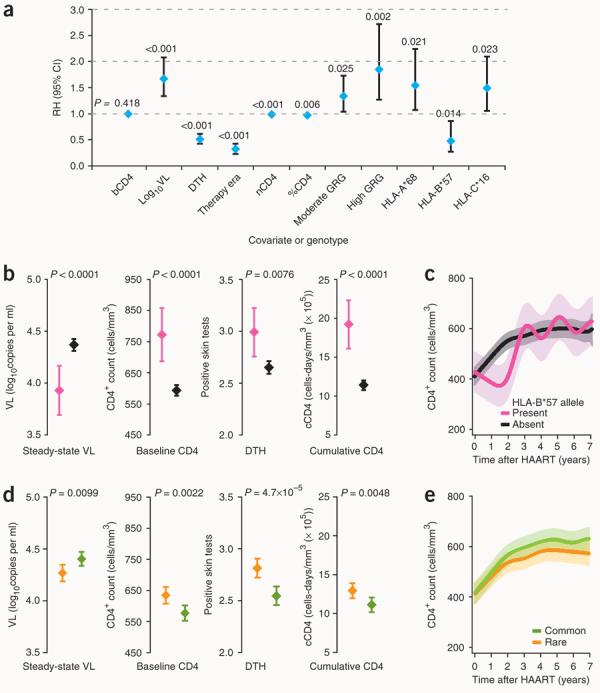
The basis for the extensive variability seen in the reconstitution of CD4(+) T cell counts in HIV-infected individuals receiving highly active antiretroviral therapy (HAART) is not fully known. Here, we show that variations in CCL3L1 gene dose and CCR5 genotype, but not major histocompatibility complex HLA alleles, influence immune reconstitution, especially when HAART is initiated at <350 CD4(+) T cells/mm(3). The CCL3L1-CCR5 genotypes favoring CD4(+) T cell recovery are similar to those that blunted CD4(+) T cell depletion during the time before HAART became available (pre-HAART era), suggesting that a common CCL3L1-CCR5 genetic pathway regulates the balance between pathogenic and reparative processes from early in the disease course. Hence, CCL3L1-CCR5 variations influence HIV pathogenesis even in the presence of HAART and, therefore, may prospectively identify subjects in whom earlier initiation of therapy is more likely to mitigate immunologic failure despite viral suppression by HAART. Furthermore, as reconstitution of CD4(+) cells during HAART is more sensitive to CCL3L1 dose than to CCR5 genotypes, CCL3L1 analogs might be efficacious in supporting immunological reconstitution.
Figures
Comment in
-
Getting personal about treating HIV.Nat Med. 2008 Apr;14(4):369-70. doi: 10.1038/nm0408-369. Nat Med. 2008. PMID: 18391933 No abstract available.
-
CCL3L1 and HIV/AIDS susceptibility.Nat Med. 2009 Oct;15(10):1110-2. doi: 10.1038/nm1009-1110. Nat Med. 2009. PMID: 19812560 Free PMC article. No abstract available.
References
-
- Douek DC, Picker LJ, Koup RA. T cell dynamics in HIV-1 infection. Annu. Rev. Immunol. 2003;21:265–304. - PubMed
-
- Rodriguez B, et al. Predictive value of plasma HIV RNA level on rate of CD4 T-cell decline in untreated HIV infection. J. Am. Med. Assoc. 2006;296:1498–1506. - PubMed
-
- Dolan MJ, et al. CCL3L1 and CCR5 influence cell-mediated immunity and affect HIV-AIDS pathogenesis via viral entry–independent mechanisms. Nat. Immunol. 2007;8:1324–1336. - PubMed
-
- Moore RD, Keruly JC. CD4+ cell count 6 years after commencement of highly active antiretroviral therapy in persons with sustained virologic suppression. Clin. Infect. Dis. 2007;44:441–446. - PubMed
-
- Grabar S, et al. Clinical outcome of patients with HIV-1 infection according to immunologic and virologic response after 6 months of highly active antiretroviral therapy. Ann. Intern. Med. 2000;133:401–410. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
