

Growth hormone, IGF-I and insulin and their abuse in sport
- PMID: 18376417
- PMCID: PMC2439509
- DOI: 10.1038/bjp.2008.99
Growth hormone, IGF-I and insulin and their abuse in sport
Abstract
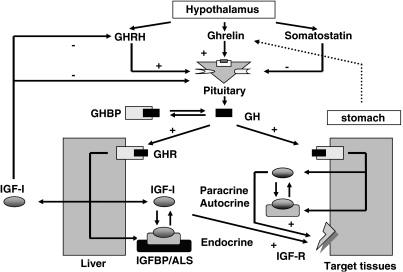
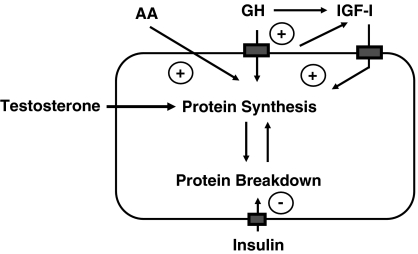
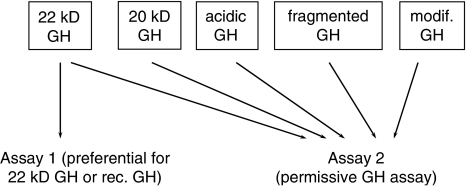
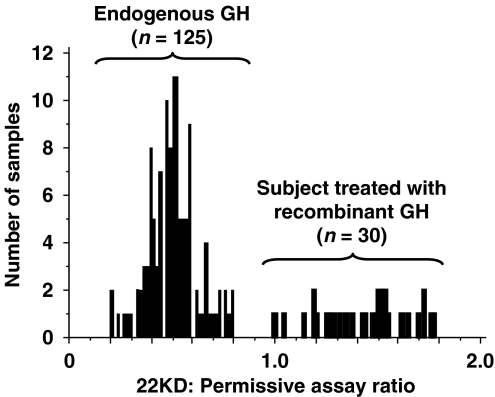
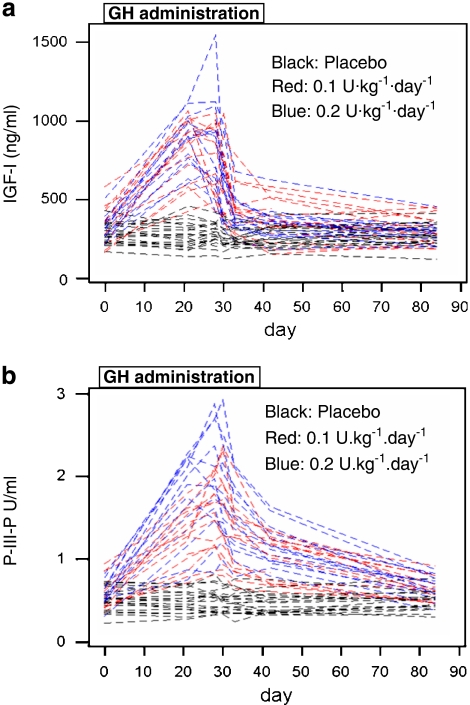
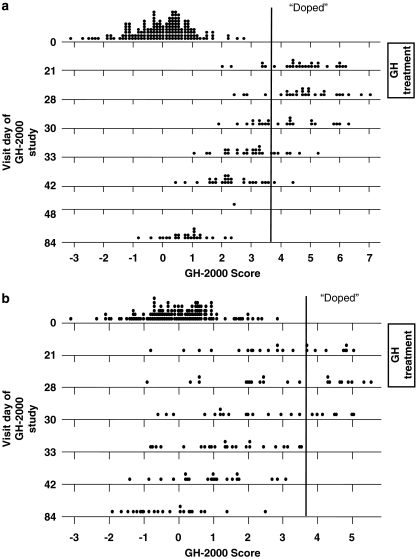
There is widespread anecdotal evidence that growth hormone (GH) is used by athletes for its anabolic and lipolytic properties. Although there is little evidence that GH improves performance in young healthy adults, randomized controlled studies carried out so far are inadequately designed to demonstrate this, not least because GH is often abused in combination with anabolic steroids and insulin. Some of the anabolic actions of GH are mediated through the generation of insulin-like growth factor-I (IGF-I), and it is believed that this is also being abused. Athletes are exposing themselves to potential harm by self-administering large doses of GH, IGF-I and insulin. The effects of excess GH are exemplified by acromegaly. IGF-I may mediate and cause some of these changes, but in addition, IGF-I may lead to profound hypoglycaemia, as indeed can insulin. Although GH is on the World Anti-doping Agency list of banned substances, the detection of abuse with GH is challenging. Two approaches have been developed to detect GH abuse. The first is based on an assessment of the effect of exogenous recombinant human GH on pituitary GH isoforms and the second is based on the measurement of markers of GH action. As a result, GH abuse can be detected with reasonable sensitivity and specificity. Testing for IGF-I and insulin is in its infancy, but the measurement of markers of GH action may also detect IGF-I usage, while urine mass spectroscopy has begun to identify the use of insulin analogues.
Figures
Similar articles
-
IGF-I abuse in sport.Curr Drug Abuse Rev. 2009 Sep;2(3):263-72. doi: 10.2174/1874473710902030263. Curr Drug Abuse Rev. 2009. PMID: 20443773 Review.
-
Beyond reasonable doubt: catching the growth hormone cheats.Pediatr Endocrinol Rev. 2007 Mar;4(3):228-32. Pediatr Endocrinol Rev. 2007. PMID: 17551486 Review.
-
[Growth hormone and IGF-1 as doping agents in competitive sport].Endokrynol Pol. 2009 Sep-Oct;60(5):389-94. Endokrynol Pol. 2009. PMID: 19885810 Review. Polish.
-
Detecting growth hormone abuse in athletes.Drug Test Anal. 2009 Sep;1(9-10):426-33. doi: 10.1002/dta.59. Drug Test Anal. 2009. PMID: 20355225 Review.
-
Insulin-like growth factor I and insulin and their abuse in sport.Endocrinol Metab Clin North Am. 2010 Mar;39(1):33-43, viii. doi: 10.1016/j.ecl.2009.10.003. Endocrinol Metab Clin North Am. 2010. PMID: 20122448
Cited by
-
The Malignant Protein Puzzle.Cerebrum. 2016 Mar 1;2016:cer-04-16. eCollection 2016 Mar-Apr. Cerebrum. 2016. PMID: 27408676 Free PMC article.
-
The Other Face of Insulin-Overdose and Its Effects.Toxics. 2022 Mar 3;10(3):123. doi: 10.3390/toxics10030123. Toxics. 2022. PMID: 35324747 Free PMC article. Review.
-
Growth hormone doping: a review.Open Access J Sports Med. 2011 Jul 27;2:99-111. doi: 10.2147/OAJSM.S11626. Open Access J Sports Med. 2011. PMID: 24198576 Free PMC article. Review.
-
Prevalence of Prohibited Substance Use and Methods by Female Athletes: Evidence of Gender-Related Differences.Front Sports Act Living. 2022 May 24;4:839976. doi: 10.3389/fspor.2022.839976. eCollection 2022. Front Sports Act Living. 2022. PMID: 35685685 Free PMC article.
-
Drug abuse in athletes.Subst Abuse Rehabil. 2014 Aug 14;5:95-105. doi: 10.2147/SAR.S53784. eCollection 2014. Subst Abuse Rehabil. 2014. PMID: 25187752 Free PMC article. Review.
References
-
- Argente J, Caballo N, Barrios V, Munoz MT, Pozo J, Chowen JA, et al. Multiple endocrine abnormalities of the growth hormone and insulin-like growth factor axis in patients with anorexia nervosa: effect of short- and long-term weight recuperation. J Clin Endocrinol Metab. 1997;82:2084–2092. - PubMed
-
- Bak JF, Moller N, Schmitz O. Effects of growth hormone on fuel utilization and muscle glycogen synthase activity in normal humans. Am J Physiol. 1991;260:736–742. - PubMed
-
- Baumann G. Growth hormone heterogeneity in human pituitary and plasma. Horm Res. 1999;51 Suppl 1:2–6. - PubMed
-
- Bidlingmaier M, Wu Z, Strasburger CJ. Problems with GH doping in sports. J Endocrinol Invest. 2003;26:924–931. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
