

"First, do no harm": monitoring outcomes during the transition from open to laparoscopic live donor nephrectomy in a Canadian centre
- PMID: 18377750
- PMCID: PMC2386338
"First, do no harm": monitoring outcomes during the transition from open to laparoscopic live donor nephrectomy in a Canadian centre
Abstract
Objective: During the learning curve for laparoscopic live donor nephrectomy (LLDN), donor morbidity and poorer graft function may be increased. To minimize these risks, a dedicated team of laparoscopic, urologic and transplant specialists worked together to introduce the technique. This study was undertaken to validate this approach by comparing donor and recipient outcomes and studying our learning curve during the transition from open (OLDN) to LLDN.
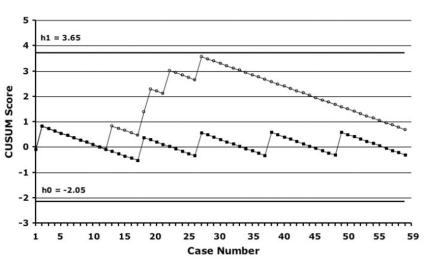
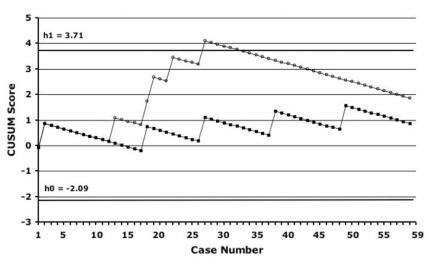
Methods: We compared 59 LLDNs with 34 OLDNs performed for adult recipients. Data were collected prospectively for LLDN and retrospectively for OLDN. We compared donor outcomes and recipient graft function in the 2 groups, and we used the cumulative sum (CUSUM) method to generate learning curves; p < 0.05 was considered statistically significant.
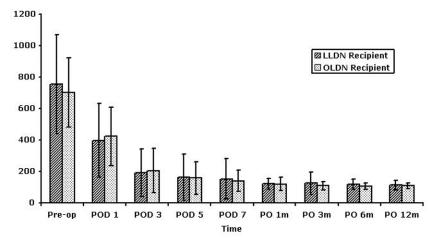
Results: From the donor standpoint, the complication rate was 10% in the laparoscopic group, compared with 21% in the open group. Length of stay was shorter after LLDN (3 v. 5 d, p < 0.001). Among the recipients, there were no significant differences in the incidences of ureteral complications, delayed graft function (DGF), creatinine levels, acute rejection or patient and graft survival. When we used the incidence of DGF after OLDN as a benchmark, CUSUM analysis revealed a downward inflection point for DGF after 30 cases, consistent with an improvement in performance.
Conclusion: At our institution, a team approach has allowed the safe introduction of LLDN without a significant negative impact on recipient outcomes and with a reduction in donor length of stay. Using DGF as an outcome, we observed improved performance after 30 cases.
Objectif: Au cours de la période d'apprentissage de la néphrectomie par laparoscopie pratiquée sur donneur vivant (NLDV), la morbidité chez le donneur et la prise moins bonne du greffon peuvent augmenter. Afin de minimiser ces risques, des spécialistes en laparoscopie, urologie et transplantation ont conjugué leur efforts en équipe pour implanter la technique. L'étude visait à valider cette approche en comparant les résultats pour les donneurs et les receveurs, et en étudiant notre courbe d'apprentissage pendant la transition de l'intervention ouverte (NODV) à l'intervention NLDV.
Méthodes: Nous avons comparé 59 NLDV et 34 NODV pratiquées pour des receveurs adultes. Nous avons recueilli les données prospectivement pour NLDV et rétrospectivement pout NODV. Nous avons comparé les résultats pour les donneurs et le fonctionnement du greffon chez les receveurs dans les deux groupes et nous avons utilisé la méthode de la somme cumulative (SUMCU) pour générer les courbes d'apprentissage. On a considéré que p < 0,05 était statistiquement significatif.
Résultats: Du point de vue des donneurs, le taux de complications s'est établi à 10 % chez ceux qui ont subi la laparoscopie comparativement à 21 % chez ceux qui ont subi l'intervention ouverte. La durée du séjour était plus courte après une NLDV (3 c. 5 j, p < 0,001). Chez les receveurs, il n'y avait pas de différences significatives au niveau des incidences des complications urétérales, du fonctionnement retardé du greffon (FRG), des taux de créatinine, du rejet aigu ou de la survie du patient et du greffon. Lorsque nous avons utilisé l'incidence du FRG après une NODV comme point de comparaison, l'analyse SUMCU a révélé un point d'inflection à la baisse dans le cas du FRG après 30 cas, ce qui concorde avec une amélioration du rendement.
Conclusion: À notre établissement, une stratégie d'équipe a permis d'implanter sans danger la NLDV sans effet négatif important sur les résultats des receveurs tout en réduisant la durée du séjour du donneur. En utilisant le FRG comme résultat, nous avons observé une amélioration du rendement après 30 cas.
Figures
Similar articles
-
Learning laparoscopic donor nephrectomy safely: a report on 100 cases.Arch Surg. 2002 May;137(5):531-4; discussion 534-5. doi: 10.1001/archsurg.137.5.531. Arch Surg. 2002. PMID: 11982464
-
Laparoscopic live donor nephrectomy: the pediatric recipient in a dual-site program.Pediatr Transplant. 2007 Jun;11(4):429-32. doi: 10.1111/j.1399-3046.2006.00664.x. Pediatr Transplant. 2007. PMID: 17493225
-
Hand-assisted laparoscopic and open living donor nephrectomy in Korea.Int J Urol. 2005 May;12(5):436-41. doi: 10.1111/j.1442-2042.2005.01086.x. Int J Urol. 2005. PMID: 15948741
-
Feasibility and safety of laparoscopic living donor nephrectomy in case of right kidney and multiple-renal artery kidney: a systematic review of the literature.World J Urol. 2020 Apr;38(4):919-927. doi: 10.1007/s00345-019-02821-8. Epub 2019 May 25. World J Urol. 2020. PMID: 31129713
-
Laparoscopic living-donor nephrectomy.Nephrol Dial Transplant. 2004 Jul;19 Suppl 4:iv36-40. doi: 10.1093/ndt/gfh1039. Nephrol Dial Transplant. 2004. PMID: 15240847 Review.
Cited by
-
Surgery through the keyhole: a new view of an old art.Mcgill J Med. 2007 Jul;10(2):140-3. Mcgill J Med. 2007. PMID: 18523542 Free PMC article. No abstract available.
-
Canadian Society of Transplantation and Canadian Society of Nephrology Commentary on the 2017 KDIGO Clinical Practice Guideline on the Evaluation and Care of Living Kidney Donors.Can J Kidney Health Dis. 2020 Jun 9;7:2054358120918457. doi: 10.1177/2054358120918457. eCollection 2020. Can J Kidney Health Dis. 2020. PMID: 32577294 Free PMC article.
-
Cumulative sum analysis score and phacoemulsification competency learning curve.Int J Ophthalmol. 2017 Jul 18;10(7):1088-1093. doi: 10.18240/ijo.2017.07.11. eCollection 2017. Int J Ophthalmol. 2017. PMID: 28730111 Free PMC article.
-
The learning curve for modified hand-assisted retroperitoneoscopic living donor nephrectomy.BMC Urol. 2024 Sep 3;24(1):191. doi: 10.1186/s12894-024-01581-x. BMC Urol. 2024. PMID: 39227858 Free PMC article.
-
Surgical complications of open nephrectomy in living related donors in Yemen: a prospective study.Turk J Urol. 2017 Dec;43(4):549-552. doi: 10.5152/tud.2017.25738. Epub 2017 Dec 1. Turk J Urol. 2017. PMID: 29201523 Free PMC article.
References
-
- Canadian Organ Replacement Register data 1997-2003 [website of the Canadian Institute of Health]. Available: http://secure.cihi.ca/cihiweb/dispPage.jsp?cw_page=statistics_results_so... (accessed 2007 Jan 7).
-
- Mange KC, Joffe MM, Feldman HI. Effect of the use or nonuse of long-term dialysis on the subsequent survival of renal transplants from living donors. N Engl J Med 2001;344:726-31. - PubMed
-
- Meier-Kriesche HU, Kaplan B. Waiting time on dialysis as the strongest modifiable risk factor for renal transplant outcomes: a paired donor kidney analysis. Transplantation 2002;74:1377-81. - PubMed
-
- Matas AJ, Bartlett ST, Leichtman AB, et al. Morbidity and mortality after living kidney donation, 1999-2001: survey of United States transplant centers. Am J Transplant 2003;3:830-4. - PubMed
-
- Kim FJ, Ratner LE, Kavoussi LR. Renal transplantation: laparoscopic live donor nephrectomy. Urol Clin North Am 2000;27:777-85. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical