

Novel systemic therapies for small cell lung cancer
- PMID: 18377849
- PMCID: PMC4086469
- DOI: 10.6004/jnccn.2008.0026
Novel systemic therapies for small cell lung cancer
Abstract
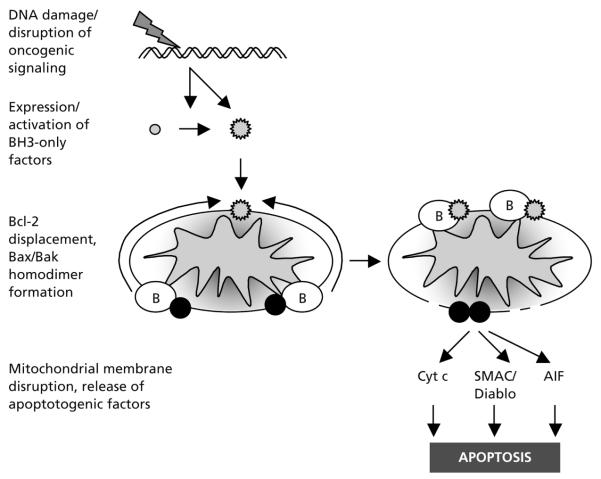
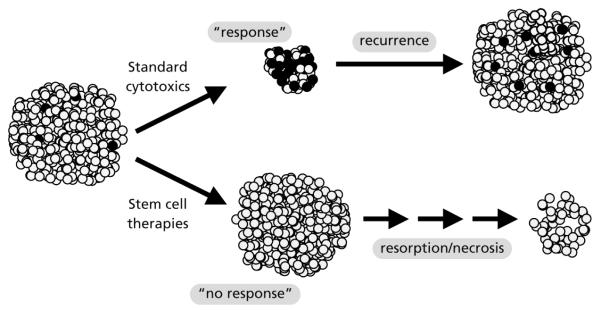
A diagnosis of small cell lung cancer (SCLC) today confers essentially the same terrible prognosis that it did 25 years ago, when common use of cisplatin-based chemotherapy began for this disease. In contrast to past decades of research on many other solid tumors, studies of combination chemotherapy using later generation cytotoxics and targeted kinase inhibitors have not had a significant impact on standard care for SCLC. The past few years have seen suggestions of incrementally improved outcomes using standard cytotoxics, including cisplatin-based combination studies of irinotecan and amrubicin by Japanese research consortia. Confirmatory phase III studies of these agents are ongoing in the United States. Antiangiogenic strategies are also of primary interest and are in late-phase testing. Several novel therapeutics, including high-potency small molecule inhibitors of Bcl-2 and the Hedgehog signaling pathway, and a recently discovered replication-competent picornavirus, have shown remarkable activity against SCLC in preclinical models and are currently in simultaneous phase I clinical development. Novel therapeutic approaches based on advances in understanding of the biology of SCLC have the potential to radically change the outlook for patients with this disease.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43–66. - PubMed
-
- Alberg AJ, Brock MV, Samet JM. Epidemiology of lung cancer: looking to the future. J Clin Oncol. 2005;23:3175–3185. - PubMed
-
- Murray N, Turrisi AT., III A review of first-line treatment for small-cell lung cancer. J Thorac Oncol. 2006;1:270–278. - PubMed
-
- Lee CB, Morris DE, Fried DB, Socinski MA. Current and evolving treatment options for limited stage small cell lung cancer. Curr Opin Oncol. 2006;18:162–172. - PubMed
-
- Murray N, Coy P, Pater JL, et al. Importance of timing for thoracic irradiation in the combined modality treatment of limited-stage small-cell lung cancer. The National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 1993;11:336–344. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
