

Using the medical record to evaluate the quality of end-of-life care in the intensive care unit
- PMID: 18379239
- PMCID: PMC2735216
- DOI: 10.1097/CCM.0b013e318168f301
Using the medical record to evaluate the quality of end-of-life care in the intensive care unit
Abstract
Rationale: We investigated whether proposed "quality markers" within the medical record are associated with family assessment of the quality of dying and death in the intensive care unit (ICU).
Objective: To identify chart-based markers that could be used as measures for improving the quality of end-of-life care.
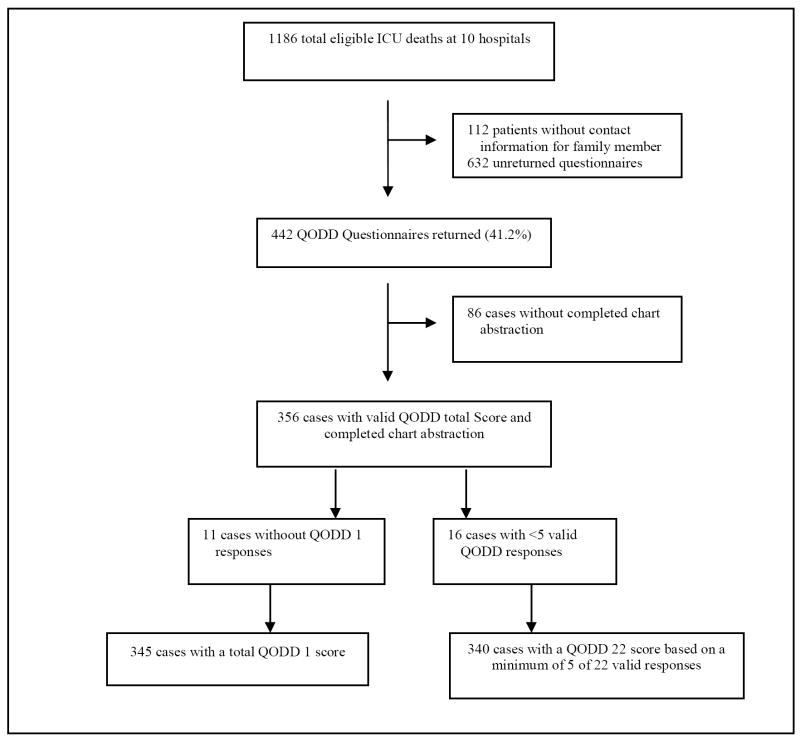
Design: A multicenter study conducting standardized chart abstraction and surveying families of patients who died in the ICU or within 24 hrs of being transferred from an ICU.
Setting: ICUs at ten hospitals in the northwest United States.
Patients: Overall, 356 patients who died in the ICU or within 24 hrs of transfer from an ICU.
Measurements: The 22-item family assessed Quality of Dying and Death (QODD-22) questionnaire and a single item rating of the overall quality of dying and death (QODD-1).
Analysis: The associations of chart-based quality markers with QODD scores were tested using Mann-Whitney U tests, Kruskal-Wallis tests, or Spearman's rank-correlation coefficients as appropriate.
Results: Higher QODD-22 scores were associated with documentation of a living will (p = .03), absence of cardiopulmonary resuscitation performed in the last hour of life (p = .01), withdrawal of tube feeding (p = .04), family presence at time of death (p = .02), and discussion of the patient's wish to withdraw life support during a family conference (p < .001). Additional correlates with a higher QODD-1 score included use of standardized comfort care orders and occurrence of a family conference (p < or = .05).
Conclusions: We identified chart-based variables associated with higher QODD scores. These QODD scores could serve as targets for measuring and improving the quality of end-of-life care in the ICU.
Figures
Comment in
-
The search for a good death--are there quality insights accessible from medical records?Crit Care Med. 2008 Apr;36(4):1372-3. doi: 10.1097/CCM.0b013e31816a11c3. Crit Care Med. 2008. PMID: 18379275 No abstract available.
References
-
- Angus DC, Barnato AE, Linde-Zwirble WT, Weissfeld LA, Watson RS, Rickert T, Rubenfeld GD. Use of intensive care at the end of life in the United States: An epidemiologic study. Crit Care Med. 2004;32:638–643. - PubMed
-
- Prendergast TJ, Claessens MT, Luce JM. A national survey of end-of-life care for critically ill patients. Am J Respir Crit Care Med. 1998;158:1163–1167. - PubMed
-
- Jayes RL, Zimmerman JE, Wagner DP, Knaus WA. Variations in the use of do-not-resuscitate orders in ICUs: findings from a national study. Chest. 1996;110:1332–1339. - PubMed
-
- Ferrand E, Robert R, Ingrand P, Lemaire F. Withholding and withdrawal of life support in intensive-care units in France: a prospective survey. Lancet. 2001;357:9–14. - PubMed
-
- Keenan SP, Busche KD, Chen LM, Esmail R, Inman KJ, Sibbald WJ. Withdrawal and withholding of life support in the intensive care unit: a comparison of teaching and community hospitals. Crit Care Med. 1998;26:245–251. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
