

Serum neutrophil gelatinase-associated lipocalin (NGAL) as a marker of acute kidney injury in critically ill children with septic shock
- PMID: 18379258
- PMCID: PMC2757115
- DOI: 10.1097/CCM.0b013e318169245a
Serum neutrophil gelatinase-associated lipocalin (NGAL) as a marker of acute kidney injury in critically ill children with septic shock
Abstract
Objective: To validate serum neutrophil gelatinase-associated lipocalin (NGAL) as an early biomarker for acute kidney injury in critically ill children with septic shock.
Design: Observational cohort study.
Setting: Fifteen North American pediatric intensive care units (PICUs).
Patients: A total of 143 critically ill children with systemic inflammatory response syndrome (SIRS) or septic shock and 25 healthy controls.
Interventions: None.
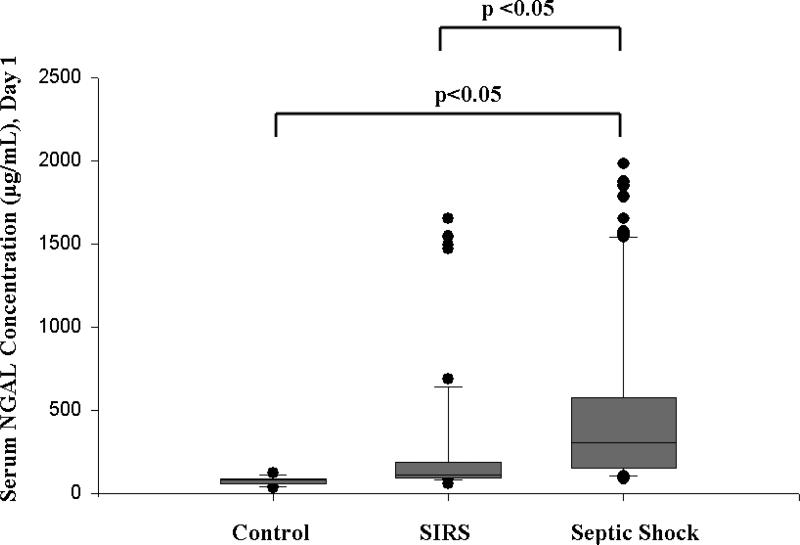
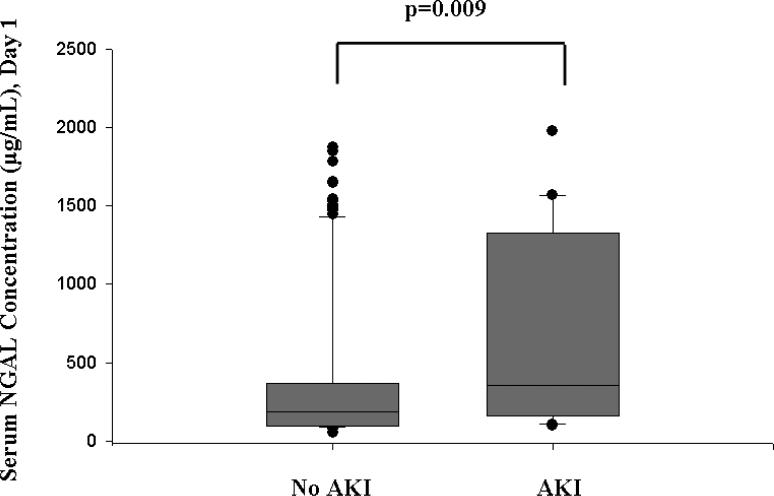
Measurements and main results: Serum NGAL was measured during the first 24 hrs of admission to the PICU. Acute kidney injury was defined as a blood urea nitrogen concentration >100 mg/dL, serum creatinine >2 mg/dL in the absence of preexisting renal disease, or the need for dialysis. There was a significant difference in serum NGAL between healthy children (median 80 ng/mL, interquartile ratio [IQR] 55.5-85.5 ng/mL), critically ill children with SIRS (median 107.5 ng/mL, IQR 89-178.5 ng/mL), and critically ill children with septic shock (median 302 ng/mL, IQR 151-570 ng/mL; p < .001). Acute kidney injury developed in 22 of 143 (15.4%) critically ill children. Serum NGAL was significantly increased in critically ill children with acute kidney injury (median 355 ng/mL, IQR 166-1322 ng/mL) compared with those without acute kidney injury (median 186 ng/mL, IQR 98-365 ng/mL; p = .009).
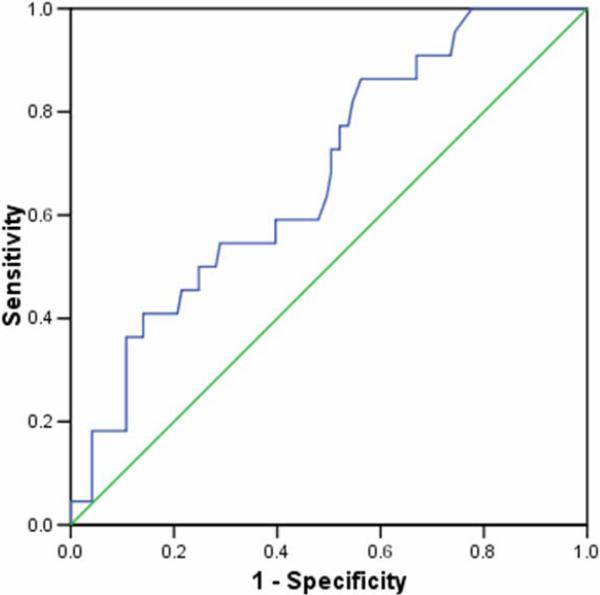
Conclusions: Serum NGAL is a highly sensitive but nonspecific predictor of acute kidney injury in critically ill children with septic shock. Further validation of serum NGAL as a biomarker of acute kidney injury in this population is warranted.
Figures
References
-
- Brivet FG, Kleinknecht DJ, Loirat P, et al. Acute renal failure in intensive care units - causes, outcome, and prognostic factors of hospital mortality: A prospective, multicenter study. French Study Group on Acute Renal Failure. Crit Care Med. 1996:192–198. - PubMed
-
- de Mendonca A, Vincent JL, Suter PM, et al. Acute renal failure in the ICU: Risk factors and outcome evaluated by the SOFA score. Intensive Care Med. 2000:915–921. - PubMed
-
- Williams DM, Sreedhar SS, Mickell JS, et al. Acute kidney failure: A pediatric experience over 20 years. Arch Pediatr Adolesc Med. 2002:893–900. - PubMed
-
- Hui-Stickle S, Brewer ED, Goldstein SL. Pediatric ARF epidemiology at a tertiary care center from 1999 to 2001. Am J Kidney Dis. 2005:96–101. - PubMed
-
- Bailey D, Phan V, Litalien C, et al. Risk factors of acute renal failure in critically ill children: A prospective descriptive epidemiological study. Pediatr Crit Care Med. 2007:29–35. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
