

Perfusion MR imaging for differentiation of benign and malignant meningiomas
- PMID: 18379768
- PMCID: PMC2440923
- DOI: 10.1007/s00234-008-0373-y
Perfusion MR imaging for differentiation of benign and malignant meningiomas
Abstract
Introduction: Our purpose was to determine whether perfusion MR imaging can be used to differentiate benign and malignant meningiomas on the basis of the differences in perfusion of tumor parenchyma and/or peritumoral edema.
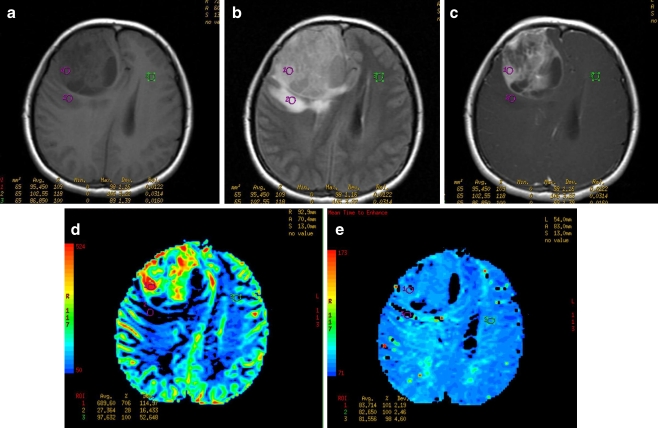
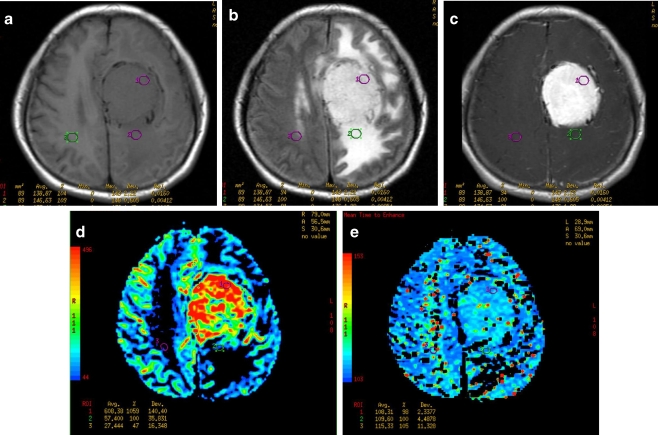
Methods: A total of 33 patients with preoperative meningiomas (25 benign and 8 malignant) underwent conventional and dynamic susceptibility contrast perfusion MR imaging. Maximal relative cerebral blood volume (rCBV) and the corresponding relative mean time to enhance (rMTE) (relative to the contralateral normal white matter) in both tumor parenchyma and peritumoral edema were measured. The independent samples t-test was used to determine whether there was a statistically significant difference in the mean rCBV and rMTE ratios between benign and malignant meningiomas.
Results: The mean maximal rCBV values of benign and malignant meningiomas were 7.16+/-4.08 (mean+/-SD) and 5.89+/-3.86, respectively, in the parenchyma, and 1.05+/-0.96 and 3.82+/-1.39, respectively, in the peritumoral edema. The mean rMTE values were 1.16+/-0.24 and 1.30+/-0.32, respectively, in the parenchyma, and 0.91+/-0.25 and 1.24+/-0.35, respectively, in the peritumoral edema. The differences in rCBV and rMTE values between benign and malignant meningiomas were not statistically significant (P>0.05) in the parenchyma, but both were statistically significant (P<0.05) in the peritumoral edema.
Conclusion: Perfusion MR imaging can provide useful information on meningioma vascularity which is not available from conventional MRI. Measurement of maximal rCBV and corresponding rMTE values in the peritumoral edema is useful in the preoperative differentiation between benign and malignant meningiomas.
Figures
Similar articles
-
Differentiation between benign and malignant meningiomas using diffusion and perfusion MR imaging.Georgian Med News. 2012 May;(206):16-22. Georgian Med News. 2012. PMID: 22870830
-
Preoperative subtyping of meningiomas by perfusion MR imaging.Neuroradiology. 2008 Oct;50(10):835-40. doi: 10.1007/s00234-008-0417-3. Epub 2008 Jun 10. Neuroradiology. 2008. PMID: 18542938
-
Contribution of dynamic contrast MR imaging to the differentiation between dural metastasis and meningioma.Neuroradiology. 2004 Aug;46(8):642-8. doi: 10.1007/s00234-004-1194-2. Epub 2004 Jun 30. Neuroradiology. 2004. PMID: 15232661 Clinical Trial.
-
Meningiomas with brain edema: radiological characteristics on MRI and review of the literature.Clin Imaging. 2002 Jul-Aug;26(4):243-9. doi: 10.1016/s0899-7071(02)00433-3. Clin Imaging. 2002. PMID: 12140153 Review.
-
Intracranial meningiomas, the VEGF-A pathway, and peritumoral brain oedema.Dan Med J. 2013 Apr;60(4):B4626. Dan Med J. 2013. PMID: 23651727 Review.
Cited by
-
ASFNR recommendations for clinical performance of MR dynamic susceptibility contrast perfusion imaging of the brain.AJNR Am J Neuroradiol. 2015 Jun;36(6):E41-51. doi: 10.3174/ajnr.A4341. Epub 2015 Apr 23. AJNR Am J Neuroradiol. 2015. PMID: 25907520 Free PMC article.
-
Alterations of cerebral microcirculation in peritumoral edema: feasibility of in vivo sidestream dark-field imaging in intracranial meningiomas.Neurooncol Adv. 2020 Aug 27;2(1):vdaa108. doi: 10.1093/noajnl/vdaa108. eCollection 2020 Jan-Dec. Neurooncol Adv. 2020. PMID: 33063011 Free PMC article.
-
Imaging of supratentorial intraventricular masses in children:a pictorial review- part 1.Neuroradiology. 2024 May;66(5):677-698. doi: 10.1007/s00234-024-03314-1. Epub 2024 Mar 11. Neuroradiology. 2024. PMID: 38466393 Free PMC article. Review.
-
Variants of meningiomas: a review of imaging findings and clinical features.Jpn J Radiol. 2016 Jul;34(7):459-69. doi: 10.1007/s11604-016-0550-6. Epub 2016 May 2. Jpn J Radiol. 2016. PMID: 27138052 Review.
-
Diffusion, Perfusion, and Histopathologic Characteristics of Desmoplastic Infantile Ganglioglioma.J Radiol Case Rep. 2016 Jul 31;10(7):1-13. doi: 10.3941/jrcr.v10i7.2715. eCollection 2016 Jul. J Radiol Case Rep. 2016. PMID: 27761184 Free PMC article. Review.
References
-
- Kleihues P, Louis DN, Scheithauer BW, Rorke LB, Reifenberger G, Burger PC, Cavenee WK. The WHO classification of tumors of the nervous system. J Neuropathol Exp Neurol. 2002;61:215–225. - PubMed
-
- Brainard JA, Prayson RA, Barnett GH. Frozen section evaluation of stereotactic brain biopsies: diagnostic yield at the stereotactic target position in 188 cases. Arch Pathol Lab Med. 1997;121:481–484. - PubMed
-
- Knopp EA, Cha S, Johnson G, Mazumdar A, Golfonos JG, Zagzag D, Kelly PJ, Kricheff II. Glial neoplasms: dynamic contrast-enhanced T2*-weighted MR imaging. Radiology. 1999;211:791–798. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
