

Noninvasive methods for determining pulmonary vascular function in children with pulmonary arterial hypertension: application of a mechanical oscillator model
- PMID: 18380759
- PMCID: PMC3116924
- DOI: 10.1111/j.1747-0803.2008.00172.x
Noninvasive methods for determining pulmonary vascular function in children with pulmonary arterial hypertension: application of a mechanical oscillator model
Abstract
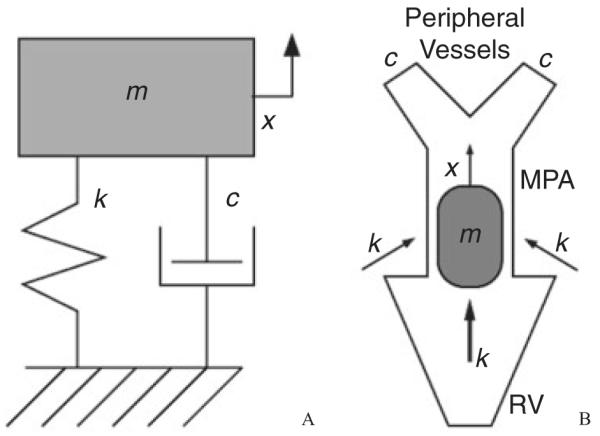
Objective: Noninvasive diagnostics for pulmonary arterial hypertension (PAH) have traditionally sought to predict main pulmonary artery pressure from qualitative or direct quantitative measures of the flow velocity pattern obtained from spectral Doppler ultrasound examination of the main pulmonary artery. A more detailed quantification of flow velocity patterns in the systemic circuit has been obtained by parameterizing the flow trace with a simple dynamic system model. Here, we investigate such a model's utility as a noninvasive predictor of total right heart afterload and right heart function.
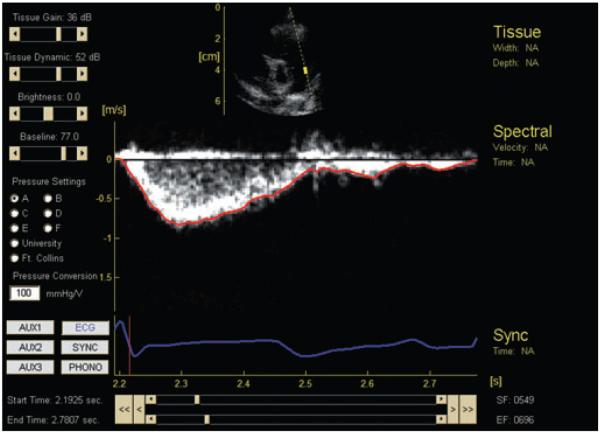
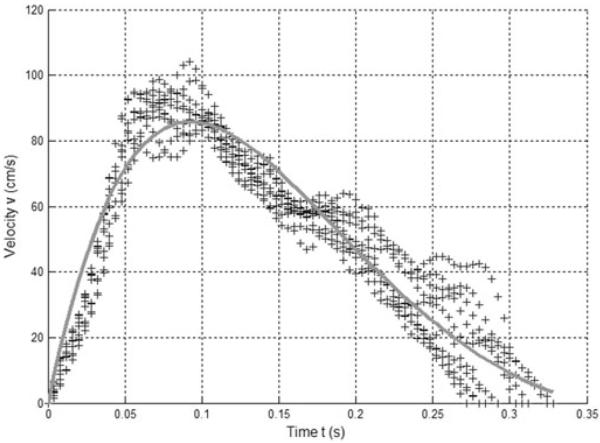
Design: Flow velocity and pressure was measured within the main pulmonary artery during right heart catheterization of patients with normal hemodynamics (19 subjects, 20 conditions) and those with PAH undergoing reactivity evaluation (34 patients, 69 conditions). Our model parameters were obtained by least-squares fitting the model velocity to the measured flow velocity.
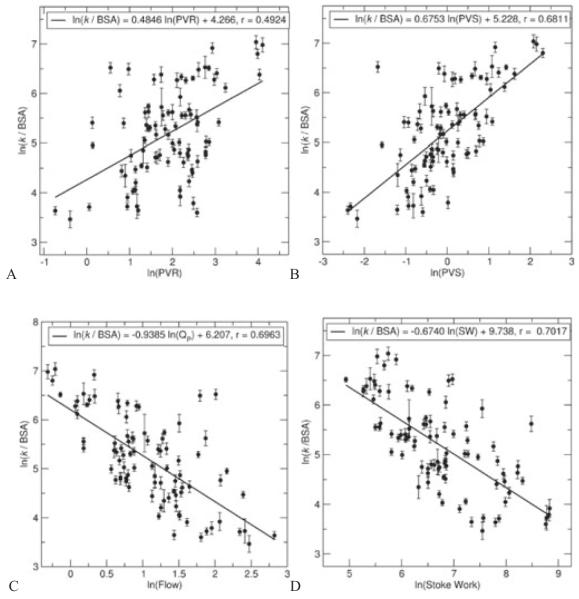
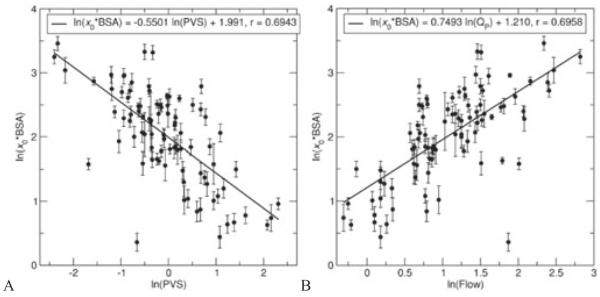
Results: Five parameter means displayed significant (P < .05) differences between normotensive and hypertensive groups. The model stiffness parameter correlated to actual pulmonary vascular resistance (r = 0.4924), pulmonary vascular stiffness (r = 0.6811), pulmonary flow (r = 0.6963), and stroke work (r = 0.7017), while the model initial displacement parameter had good correlation to stiffness (r = 0.6943) and flow (r = 0.6958).
Conclusions: As predictors of total right heart afterload (resistance and stiffness) and right ventricle work, the model parameters of stiffness and initial displacement offer more comprehensive measures of the disease state than previous noninvasive methods and may be useful in routine diagnostic monitoring of patients with PAH.
Figures
References
-
- Ivy DD. Echocardiographic evaluation of pulmonary hypertension. In: Valdes-Cruz LM, Cayre RO, editors. Echocardiography Diagnosis of Congenital Heart Disease: An Embryologic and Anatomic Approach. Lippincott-Raven; Philadelphia: 1999. pp. 537–547.
-
- Kitabatake A, Inoue M, Asao M, et al. Noninvasive evaluation of pulmonary hypertension by a pulsed Doppler technique. Circulation. 1983;68:302–309. - PubMed
-
- Dabestani A, Mahan G, Gardin JM, et al. Evaluation of pulmonary artery pressure and resistance by pulsed Doppler echocardiography. Am J Cardiol. 1987;59:662–668. - PubMed
-
- Martin-Duran R, Larman M, Trugeda A, et al. Comparison of Doppler-determined elevated pulmonary arterial pressure with pressure measured at cardiac catheterization. Am J Cardiol. 1986;57:859–863. - PubMed
-
- Kosturakis D, Goldberg SJ, Allen HD, Loeber C. Doppler echocardiographic prediction of pulmonary arterial hypertension in congenital heart disease. Am J Cardiol. 1984;53:1110–1115. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
