

Early diagnosis of neuropathy in leprosy--comparing diagnostic tests in a large prospective study (the INFIR cohort study)
- PMID: 18382604
- PMCID: PMC2270341
- DOI: 10.1371/journal.pntd.0000212
Early diagnosis of neuropathy in leprosy--comparing diagnostic tests in a large prospective study (the INFIR cohort study)
Abstract
Background: Leprosy is the most frequent treatable neuromuscular disease. Yet, every year, thousands of patients develop permanent peripheral nerve damage as a result of leprosy. Since early detection and treatment of neuropathy in leprosy has strong preventive potential, we conducted a cohort study to determine which test detects this neuropathy earliest.
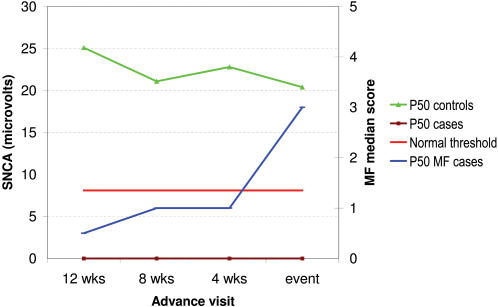
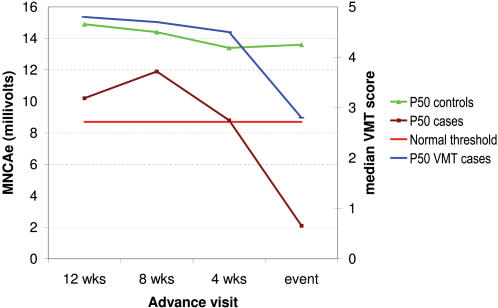
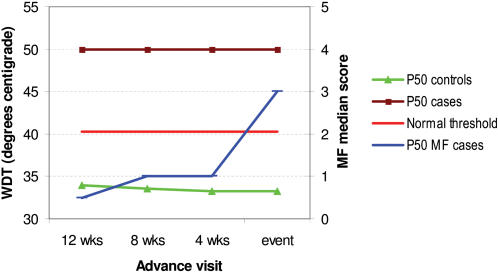
Methods and findings: One hundred and eighty-eight multibacillary (MB) leprosy patients were selected from a cohort of 303 and followed for 2 years after diagnosis. Nerve function was evaluated at each visit using nerve conduction (NC), quantitative thermal sensory testing and vibrometry, dynamometry, monofilament testing (MFT), and voluntary muscle testing (VMT). Study outcomes were sensory and motor impairment detected by MFT or VMT. Seventy-four of 188 patients (39%) had a reaction, neuritis, or new nerve function impairment (NFI) event during a 2-year follow-up. Sub-clinical neuropathy was extensive (20%-50%), even in patients who did not develop an outcome event. Sensory nerve action potential (SNAP) amplitudes, compound motor action potential (CMAP) velocities, and warm detection thresholds (WDT) were most frequently affected, with SNAP impairment frequencies ranging from 30% (median) to 69% (sural). Velocity was impaired in up to 43% of motor nerves. WDTs were more frequently affected than cold detection thresholds (29% versus 13%, ulnar nerve). Impairment of SNC and warm perception often preceded deterioration in MF or VMT scores by 12 weeks or more.
Conclusions: A large proportion of leprosy patients have subclinical neuropathy that was not evident when only MFT and VMT were used. SNC was the most frequently and earliest affected test, closely followed by WDT. They are promising tests for improving early detection of neuropathy, as they often became abnormal 12 weeks or more before an abnormal monofilament test. Changes in MFT and VMT score mirrored changes in neurophysiology, confirming their validity as screening tests.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Nicholls PG, Croft RP, Richardus JH, Withington SG, Smith WC. Delay in presentation, an indicator for nerve function status at registration and for treatment outcome–the experience of the Bangladesh Acute Nerve Damage Study cohort. Lepr Rev. 2003;74:349–356. - PubMed
-
- Meima A, Saunderson PR, Gebre S, Desta K, van Oortmarssen GJ, Habbema JD. Factors associated with impairments in new leprosy patients: the AMFES cohort [In Process Citation]. Lepr Rev. 1999;70:189–203. - PubMed
-
- Van Veen NH, Meima A, Richardus JH. The relationship between detection delay and impairment in leprosy control: a comparison of patient cohorts from Bangladesh and Ethiopia. Lepr Rev. 2006;77:356–365. - PubMed
-
- Schreuder PA. The occurrence of reactions and impairments in leprosy: experience in the leprosy control program of three provinces in northeastern Thailand, 1987–1995 [correction of 1978–1995]. III. Neural and other impairments. Int J Lepr Other Mycobact Dis. 1998;66:170–181. - PubMed
-
- Reed NK, van Brakel WH, Reed DS. Progress of impairment scores following commencement of chemotherapy in multibacillary leprosy patients. Int J Lepr Other Mycobact Dis. 1997;65:328–336. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
