

A randomised, blinded, placebo-controlled trial in dementia patients continuing or stopping neuroleptics (the DART-AD trial)
- PMID: 18384230
- PMCID: PMC2276521
- DOI: 10.1371/journal.pmed.0050076
A randomised, blinded, placebo-controlled trial in dementia patients continuing or stopping neuroleptics (the DART-AD trial)
Abstract
Background: There have been increasing concerns regarding the safety and efficacy of neuroleptics in people with dementia, but there are very few long-term trials to inform clinical practice. The aim of this study was to determine the impact of long-term treatment with neuroleptic agents upon global cognitive decline and neuropsychiatric symptoms in patients with Alzheimer disease.
Design: Randomised, blinded, placebo-controlled parallel two-group treatment discontinuation trial.
Setting: Oxfordshire, Newcastle and Gateshead, London and Edinburgh, United Kingdom.
Participants: Patients currently prescribed the neuroleptics thioridazine, chlorpromazine, haloperidol trifluoperazine or risperidone for behavioural or psychiatric disturbance in dementia for at least 3 mo.
Interventions: Continue neuroleptic treatment for 12 mo or switch to an identical placebo.
Outcome measures: Primary outcome was total Severe Impairment Battery (SIB) score. Neuropsychiatric symptoms were evaluated with the Neuropsychiatric Inventory (NPI).
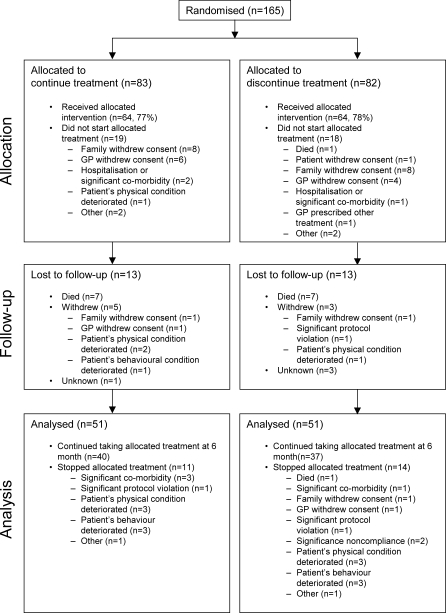
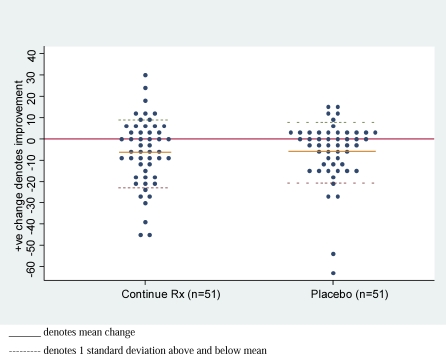
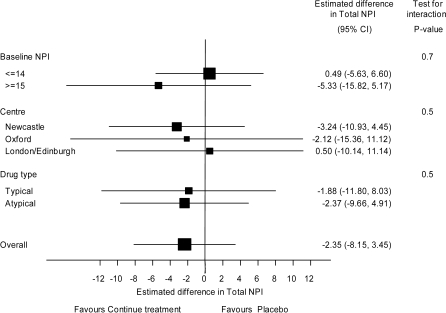
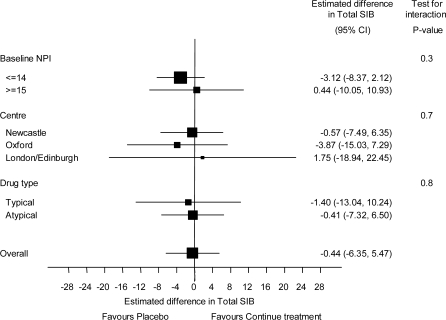
Results: 165 patients were randomised (83 to continue treatment and 82 to placebo, i.e., discontinue treatment), of whom 128 (78%) commenced treatment (64 continue/64 placebo). Of those, 26 were lost to follow-up (13 per arm), resulting in 51 patients per arm analysed for the primary outcome. There was no significant difference between the continue treatment and placebo groups in the estimated mean change in SIB scores between baseline and 6 mo; estimated mean difference in deterioration (favouring placebo) -0.4 (95% confidence interval [CI] -6.4 to 5.5), adjusted for baseline value (p = 0.9). For neuropsychiatric symptoms, there was no significant difference between the continue treatment and placebo groups (n = 56 and 53, respectively) in the estimated mean change in NPI scores between baseline and 6 mo; estimated mean difference in deterioration (favouring continue treatment) -2.4 (95% CI -8.2 to 3.5), adjusted for baseline value (p = 0.4). Both results became more pronounced at 12 mo. There was some evidence to suggest that those patients with initial NPI >/= 15 benefited on neuropsychiatric symptoms from continuing treatment.
Conclusions: For most patients with AD, withdrawal of neuroleptics had no overall detrimental effect on functional and cognitive status. Neuroleptics may have some value in the maintenance treatment of more severe neuropsychiatric symptoms, but this benefit must be weighed against the side effects of therapy.
Trial registration: Cochrane Central Registry of Controlled Trials/National Research Register (#ISRCTN33368770).
Conflict of interest statement
Figures
Comment in
-
Neuroleptic discontinuation during dementia care: a recent trial and its implications for practice.Nat Clin Pract Neurol. 2008 Oct;4(10):528-9. doi: 10.1038/ncpneuro0884. Epub 2008 Aug 26. Nat Clin Pract Neurol. 2008. PMID: 18725920 No abstract available.
References
-
- Ballard C, Ayre G, Gray A. Psychotic symptoms and behavioral disturbances in dementia: A review. Rev Neurol. 1999;155:44–52. - PubMed
-
- Gilley DW, Whalen ME, Wilson RS, Bennett DA. Hallucinations and associated factors in Alzheimer's disease. J Neuropsych Clin Neurosci. 1991;3:371–376. - PubMed
-
- Rabins PV, Mace NL, Lucas MJ. The impact of dementia on the family. J Am Med Soc. 1982;248:333–335. - PubMed
-
- Donaldson C, Tarrier N, Burns A. The impact of the symptoms of dementia on caregivers. Brit J Psychiatr. 1997;170:62–68. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
