

Risk factors for the development of nosocomial pneumonia and mortality on intensive care units: application of competing risks models
- PMID: 18384672
- PMCID: PMC2447589
- DOI: 10.1186/cc6852
Risk factors for the development of nosocomial pneumonia and mortality on intensive care units: application of competing risks models
Abstract
Introduction: Pneumonia is a very common nosocomial infection in intensive care units (ICUs). Many studies have investigated risk factors for the development of infection and its consequences. However, the evaluation in most of theses studies disregards the fact that there are additional competing events, such as discharge or death.
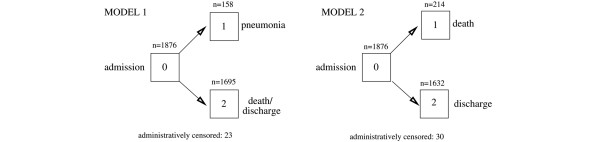
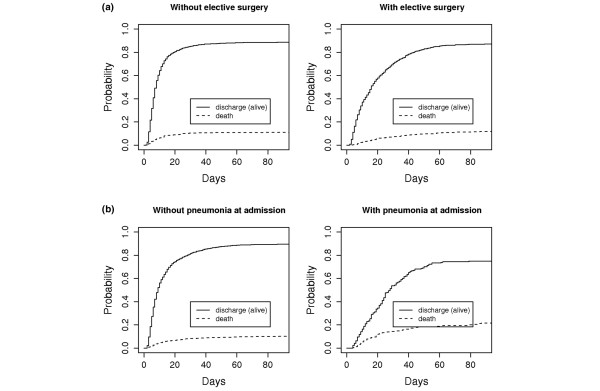
Methods: A prospective cohort study was conducted over 18 months in five intensive care units at one university hospital. All patients that were admitted for at least 2 days were included, and surveillance of nosocomial pneumonia was conducted. Various potential risk factors (baseline- and time-dependent) were evaluated in two competing risks models: the acquisition of nosocomial pneumonia and discharge (dead or alive; model 1) and for the risk of death in the ICU and discharge alive (model 2).
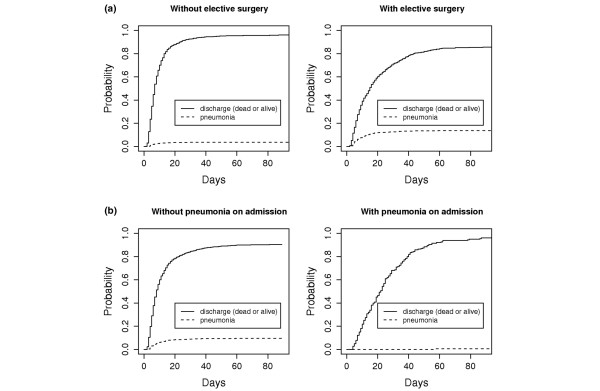
Results: Patients from 1,876 admissions were included. A total of 158 patients developed nosocomial pneumonia. The main risk factors for nosocomial pneumonia in the multivariate analysis in model 1 were: elective surgery (cause-specific hazard ratio = 1.95; 95% CI 1.33 to 2.85) or emergency surgery (1.59; 95% CI 1.10 to 2.28) prior to ICU admission, usage of a nasogastric tube (3.04; 95% CI 1.25 to 7.37) and mechanical ventilation (5.90; 95% CI 2.47 to 14.09). Nosocomial pneumonia prolonged the length of ICU stay but was not directly associated with a fatal outcome (p = 0.55).
Conclusion: More studies using competing risk models, which provide more accurate data compared to naive survival curves or logistic models, should be carried out to verify the impact of risk factors and patient characteristics for the acquisition of nosocomial infections and infection-associated mortality.
Figures
Comment in
-
Competing risks models and time-dependent covariates.Crit Care. 2008;12(2):134. doi: 10.1186/cc6840. Epub 2008 Apr 11. Crit Care. 2008. PMID: 18423067 Free PMC article.
References
-
- Cook DJ, Walter SD, Cook RJ, Griffith LE, Guyatt GH, Leasa D, Jaeschke RZ, Brun-Buisson C. Incidence of and risk factors for ventilator-associated pneumonia in critically ill patients. Ann Intern Med. 1998;129:433–440. - PubMed
-
- Meric M, Willke A, Caglayan C, Toker K. Intensive care unit-acquired infections: incidence, risk factors and associated mortality in a Turkish university hospital. Jpn J Infect Dis. 2005;58:297–302. - PubMed
-
- Apostolopoulou E, Bakakos P, Katostaras T, Gregorakos L. Incidence and risk factors for ventilator-associated pneumonia in 4 multidisciplinary intensive care units in Athens, Greece. Respir Care. 2003;48:681–688. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
