

Peripheral virus-specific T-cell interleukin-10 responses develop early in acute hepatitis C infection and become dominant in chronic hepatitis
- PMID: 18384906
- PMCID: PMC2430081
- DOI: 10.1016/j.jhep.2008.01.030
Peripheral virus-specific T-cell interleukin-10 responses develop early in acute hepatitis C infection and become dominant in chronic hepatitis
Abstract
Background/aims: Interleukin-10 (IL-10) has been ascribed pro-viral but anti-fibrotic properties in chronic hepatitis C virus (HCV) infection. In this study, we examined the role of HCV-specific T-cell IL-10 response in patients with acute and chronic HCV infection.
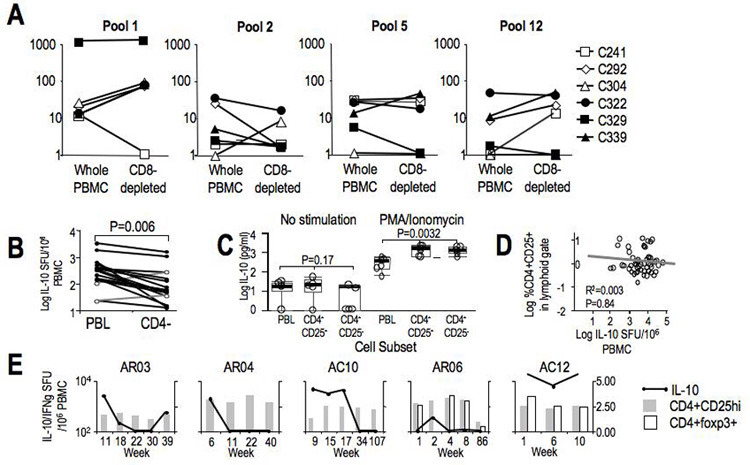
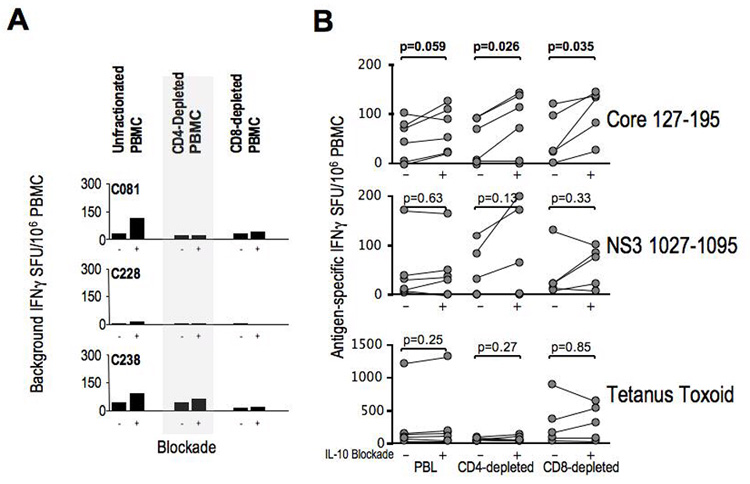
Methods: Peripheral HCV-specific T-cell IL-10 and IFNgamma responses were measured in cytokine Elispot assay using overlapping HCV-derived peptides in patients with chronic (n=61), resolved (n=15) and acute (n=8) hepatitis C, looking for their onset, quantity, breadth and durability relative to clinical and virological outcomes. The source and effect of HCV-specific IL-10 response were determined in depletion and IL-10 neutralization experiments.
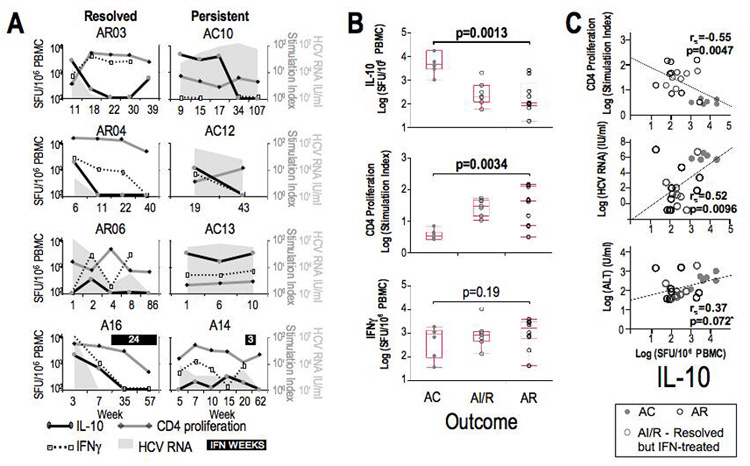
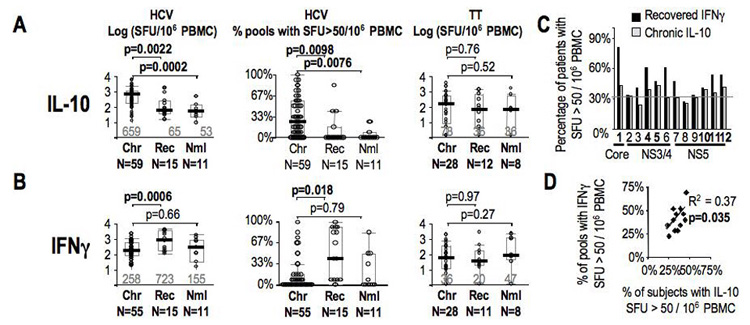
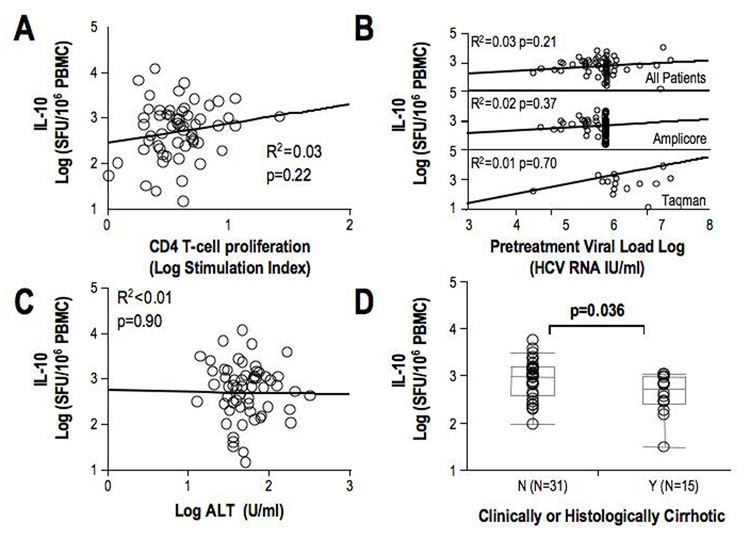
Results: Both HCV-specific IL-10 and IFNgamma responses were detected early within 1-2 months of acute clinical hepatitis C. However, only HCV-specific IL-10 response correlated with elevated liver enzymes, increased viremia and suppressed HCV-specific CD4(+) T-cell proliferation in acute infection. While these associations were lost in established chronic infection, HCV-specific IL-10 responses were increased in patients without cirrhosis while IL-10 blockade enhanced antiviral effector IFNgamma responses.
Conclusions: HCV-specific IL-10 Tr1 responses may play a dual role in HCV infection, dampening effector T-cells to promote viral persistence in acute infection but also protecting against progressive fibrosis in chronic infection.
Figures
References
-
- Takaki A, Wiese M, Maertens G, Depla E, Seifert U, Liebetrau A, et al. Cellular immune responses persist and humoral responses decrease two decades after recovery from a single-source outbreak of hepatitis C. Nat Med. 2000;6:578–582. - PubMed
-
- Chang KM, Thimme R, Melpolder JJ, Oldach D, Pemberton J, Moorhead-Loudis J, et al. Differential CD4(+) and CD8(+) T-cell responsiveness in hepatitis C virus infection. Hepatology. 2001;33:267–276. - PubMed
-
- Wedemeyer H, He XS, Nascimbeni M, Davis AR, Greenberg HB, Hoofnagle JH, et al. Impaired effector function of hepatitis C virus-specific CD8+ T cells in chronic hepatitis C virus infection. J Immunol. 2002;169:3447–3458. - PubMed
-
- Ulsenheimer A, Gerlach JT, Gruener NH, Jung MC, Schirren CA, Schraut W, et al. Detection of functionally altered hepatitis C virus-specific CD4 T cells in acute and chronic hepatitis C. Hepatology. 2003;37:1189–1198. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01-AI-47519/AI/NIAID NIH HHS/United States
- K12-RR-017625/RR/NCRR NIH HHS/United States
- R01-AA-12849/AA/NIAAA NIH HHS/United States
- R01 AI047519/AI/NIAID NIH HHS/United States
- L30 DK069063/DK/NIDDK NIH HHS/United States
- K12 RR017625/RR/NCRR NIH HHS/United States
- P30DK50306/DK/NIDDK NIH HHS/United States
- T32 DK007066/DK/NIDDK NIH HHS/United States
- R01 AA012849/AA/NIAAA NIH HHS/United States
- P30 DK050306/DK/NIDDK NIH HHS/United States
- M01 RR000040/RR/NCRR NIH HHS/United States
- T32 DK 07066/DK/NIDDK NIH HHS/United States
- M01-RR00040/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
