

Nonpalpable breast masses: evaluation by US elastography
- PMID: 18385557
- PMCID: PMC2627231
- DOI: 10.3348/kjr.2008.9.2.111
Nonpalpable breast masses: evaluation by US elastography
Abstract
Objective: To compare the diagnostic performances of conventional ultrasound (US) and US elastography for the differentiation of nonpalpable breast masses, and to evaluate whether elastography is helpful at reducing the number of benign biopsies, using histological analysis as a reference standard.
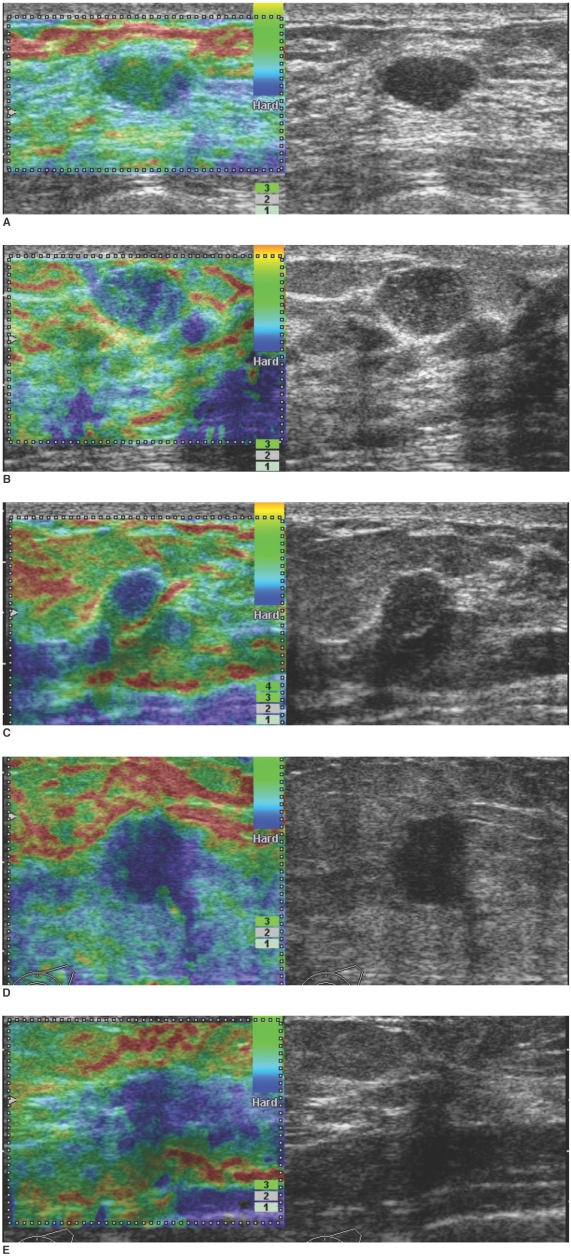
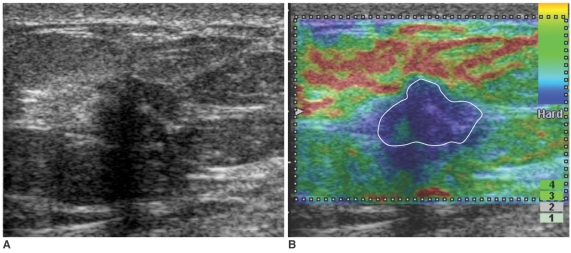
Materials and methods: Conventional US and real-time elastographic images were obtained for 100 women who had been scheduled for a US-guided core biopsy of 100 nonpalpable breast masses (83 benign, 17 malignant). Two experienced radiologists unaware of the biopsy and clinical findings analyzed conventional US and elastographic images by consensus, and classified lesions based on degree of suspicion regarding the probability of malignancy. Results were evaluated by receiver operating characteristic curve analysis. In addition, the authors investigated whether a subset of lesions was categorized as suspicious by conventional US, but as benign by elastography.
Results: Areas under the ROC curves (Az values) were 0.901 for conventional US and 0.916 for elastography (p = 0.808). For BI-RADS category 4a lesions, 44% (22 of 50) had an elasticity score of 1 and all were found to be benign.
Conclusion: Elastography was found to have a diagnostic performance comparable to that of conventional US for the differentiation of nonpalpable breast masses. The authors conclude that BI-RADS category 4a lesions with an elasticity score of 1 probably do not require biopsy.
Figures


References
-
- Stavros AT, Thickman D, Rapp CL, Dennis MA, Parker SH, Sisney GA. Solid breast nodules: use of sonography to distinguish between benign and malignant lesions. Radiology. 1995;196:123–134. - PubMed
-
- Rahbar G, Sie AC, Hansen GC, Prince JS, Melany ML, Reynolds HE, et al. Benign versus malignant solid breast masses: US differentiation. Radiology. 1999;213:889–894. - PubMed
-
- Park SY, Oh KK, Kim EK, Son EJ, Chung WH. Sonographic findings of breast hamartoma: emphasis on compressibility. Yonsei Med J. 2003;44:847–854. - PubMed
-
- Steinberg BD, Sullivan DC, Carlson DL. Disparity mapping applied to sonography of the breast: technical note. Radiology. 1998;207:545–550. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
