

Intrapancreatic accessory spleen: findings on MR Imaging, CT, US and scintigraphy, and the pathologic analysis
- PMID: 18385564
- PMCID: PMC2627219
- DOI: 10.3348/kjr.2008.9.2.162
Intrapancreatic accessory spleen: findings on MR Imaging, CT, US and scintigraphy, and the pathologic analysis
Abstract
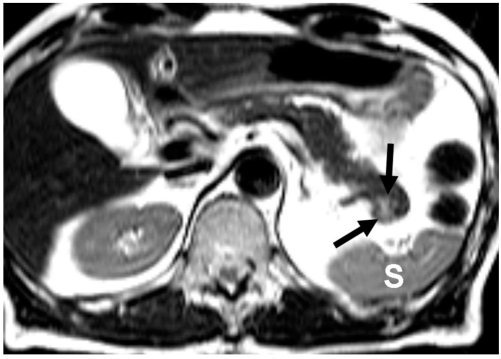
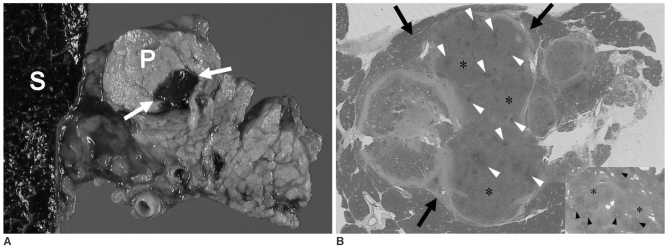
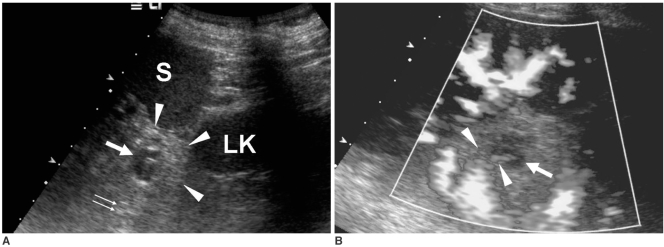
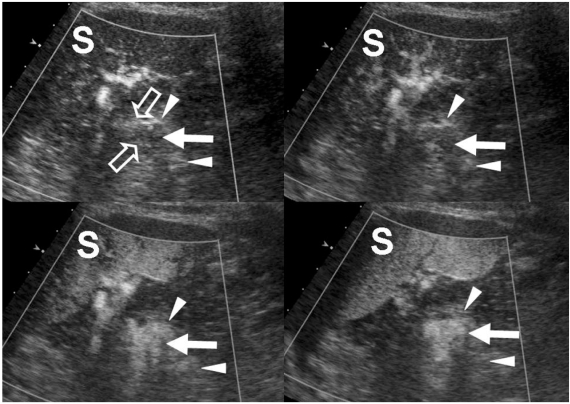
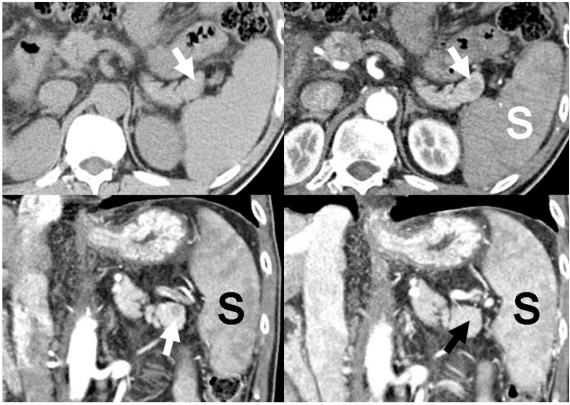
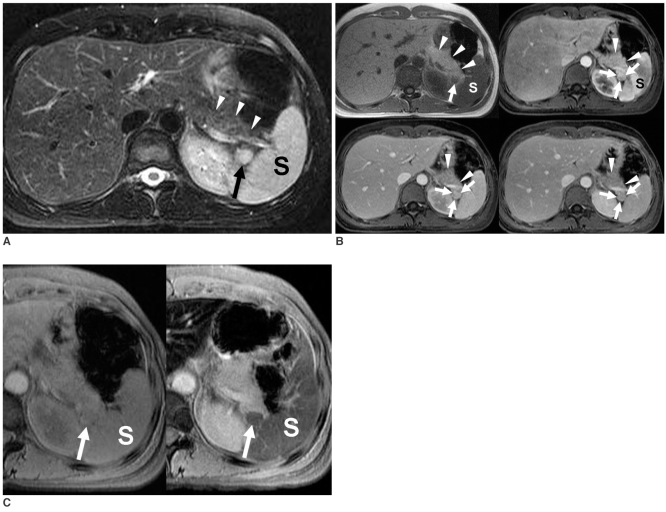
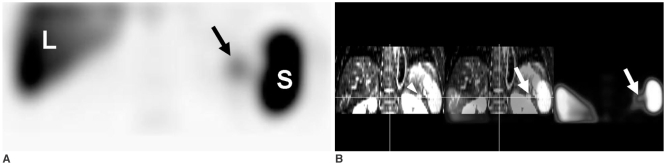
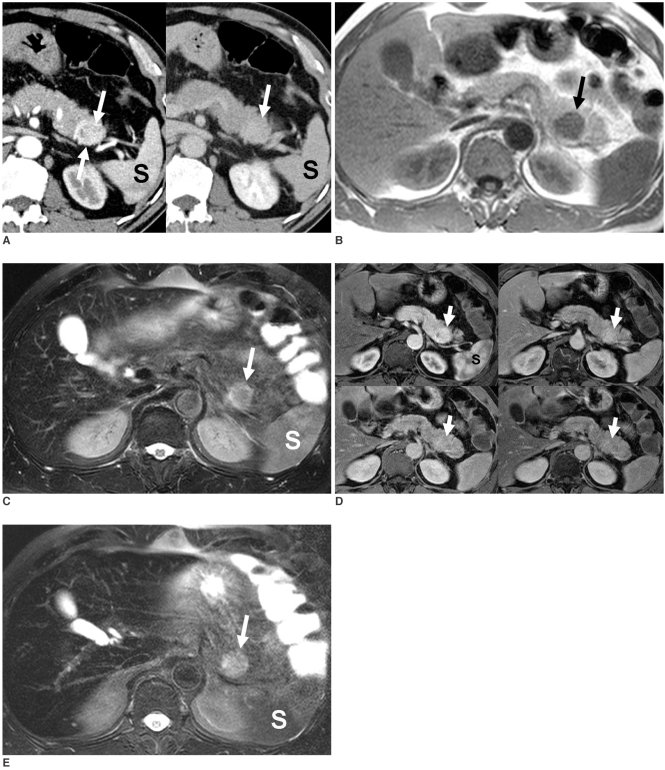
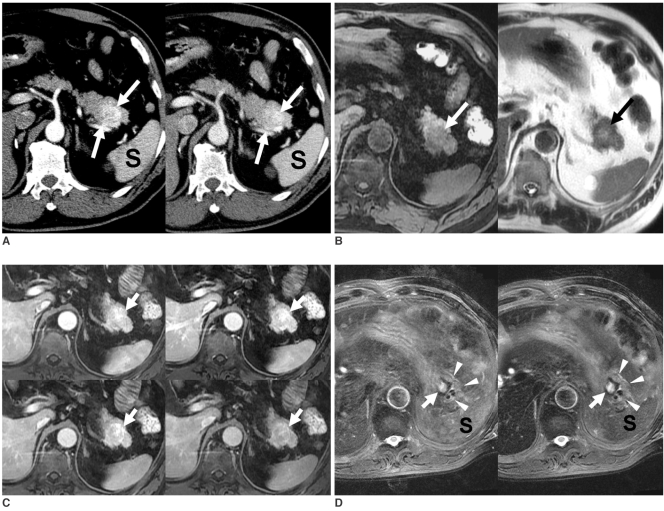
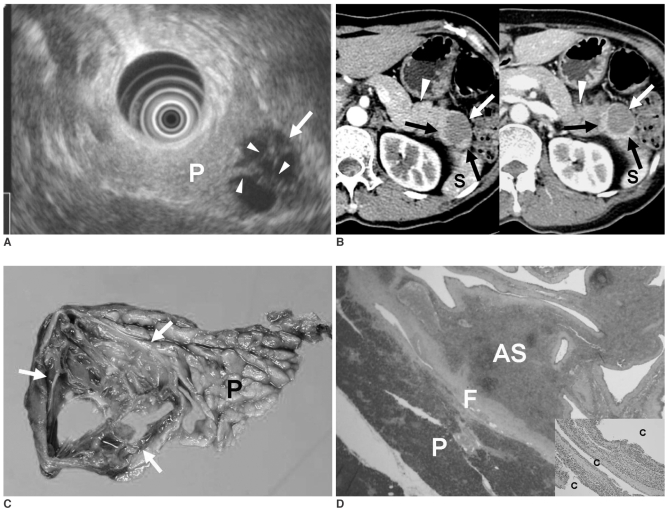
Although the tail of the pancreas is the second most common site of an accessory spleen, intrapancreatic accessory spleen (IPAS) has rarely been noted radiologically. However, as the imaging techniques have recently advanced, IPAS will be more frequently detected as an incidental pancreatic nodule on CT or MRI. Because accessory spleens usually pose no clinical problems, it is important to characterize accessory spleens as noninvasively as possible. An IPAS has similar characteristics to those of the spleen on the precontrast and contrast-enhanced images of all the imaging modalities. In particular, inhomogeneous enhancement of an IPAS in its early phases may be a diagnostic clue. Superparamagnetic iron oxide (SPIO)-enhanced MRI and Levovist-enhanced US, and the mechanisms of which are theoretically similar to that of Tc-99m scintigraphy, can be used as alternative tools to confirm the diagnosis of IPAS. An IPAS shows a significant signal drop similar to the spleen on the SPIO-enhanced T2 or T2*-weighted imaging and prolonged enhancement on the delayed hepatosplenic phase of contrast-enhanced US. We review and illustrate the differential points between IPAS and hypervascular pancreatic tumors in this manuscript.
Figures

References
-
- Movitz D. Accessory spleens and experimental splenosis. Principles of growth. Chic Med Sch Q. 1967;26:183–187. - PubMed
-
- Halpert B, Gyorkey F. Lesions observed in accessory spleens of 311 patients. Am J Clin Pathol. 1959;32:165–168. - PubMed
-
- Eraklis AJ, Filler RM. Splenectomy in childhood: a review of 1413 cases. J Pediatr Surg. 1972;7:382–388. - PubMed
-
- Harris GN, Kase DJ, Bradnock H, Mckinley MJ. Accessory spleen causing a mass in the tail of the pancreas: MR imaging findings. AJR Am J Roentgenol. 1994;163:1120–1121. - PubMed
-
- Hamada T, Isaji S, Mizuno S, Tabata M, Yamagiwa K, Yokoi H, et al. Laparoscopic spleen-preserving pancreatic tail resection for an intrapancreatic accessory spleen mimicking a nonfunctioning endocrine tumor: report of a case. Surg Today. 2004;34:878–881. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
