

Prostate stem cells and benign prostatic hyperplasia
- PMID: 18386293
- PMCID: PMC3350783
- DOI: 10.1002/pros.20763
Prostate stem cells and benign prostatic hyperplasia
Abstract
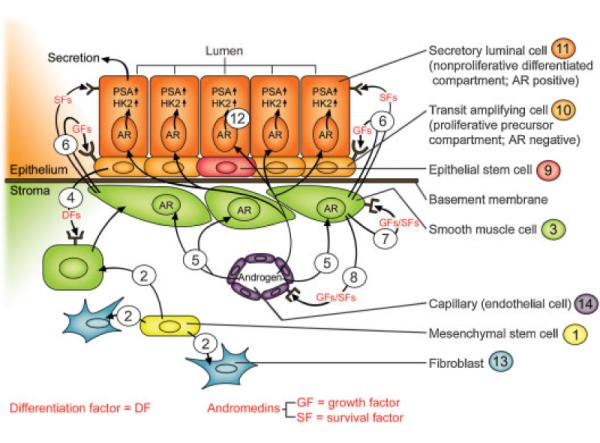
Pharmacological approaches are available to medically-managed patients with symptomatic BPH before surgical intervention is required. These include daily treatment with alpha-blockers and 5-alpha-reductase inhibitors alone or in combination. These medical approaches have two major problems. First, treatments are chronic and must be taken daily. Second, there are significant financial costs and quality of life issues for such chronic treatments. Is it possible to develop effective acute therapy for symptomatic BPH without the long-term androgen deprivation-induced side effects? Two seminal but rarely cited studies of Walsh [Peters, Walsh: N Engl J Med 317:599-604, 1987] and Coffey et al. [Sufrin et al.: Invest Urol 13:418-423, 1976], combined with the growing understanding of the stem cell organization of the prostate stromal (S) and epithelial (E) compartments and their reciprocal paracrine and autocrine interactions provides the rationale for an acute approach.The Walsh study documents that: (1) androgen deprivation disrupts the reciprocal interaction between the prostate S and E thereby decreasing the weight of both compartments and (2) once BPH develops, androgen deprivation does not decrease the number of stem cell units in either the S or E compartments since subsequent androgen restoration fully restores the enlarged gland. The Coffey study documents that acute androgen deprivation sensitizes S-E interactions to radiation induced disruptions so that following radiation, androgen restoration does not induce full gland regrowth. Therefore, effective therapy for symptomatic BPH should be achievable by acute treatment with reversible androgen deprivation for a limited period followed by a single dose of conformal external beam radiation before allowing the man to recovery his normal serum testosterone.
Figures
References
-
- Nasland MJ, Miner M. A Review of the Clinical Efficacy and Safety of 5alpha- Reductase Inhibitors for the Enlarged Prostate. Clin Ther. 2007;29:17–25. - PubMed
-
- Roehrborn CG, McConnell JD, Lieber M, Kaplan S, Geller J, Malek GH, Castellanos R, Coffield S, Saltzman B, Resnick M, Cook TJ, Waldstreicher J. Serum prostate-specific antigen concentration is a powerful predictor of acute urinary retension and need for surgery in men with clinical benign prostatic hyperplasia. Urology. 1999;53:473–480. - PubMed
-
- Boyle P, Roehrborn C, Harkaway R, Logie J, de la Rosette J, Emberton M. %-Alpha reductase inhibition provides superior benefits to alpha blockade by preventing AUR and BPH-related surgery. Eur Urol. 2004;45:620–626. - PubMed
-
- Souverein PC, Erkens JA, de la Rosette JJ, Leufkens HG, Herings RM. Drug treatment of benign prostatic hyperplasia and hospital admission for BPH-related surgery. Eur Urol. 2003;43:528–534. - PubMed
-
- Litvinov IV, De Marzo AM, Isaacs JT. Is the Achilles's heel for prostate cancer therapy a gain of function in androgen receptor signaling? J Clin Endocrinol Metab. 2003;88:2972–2982. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
