

Do variations in provider discussions explain socioeconomic disparities in postmastectomy breast reconstruction?
- PMID: 18387464
- PMCID: PMC4002201
- DOI: 10.1016/j.jamcollsurg.2007.11.017
Do variations in provider discussions explain socioeconomic disparities in postmastectomy breast reconstruction?
Abstract
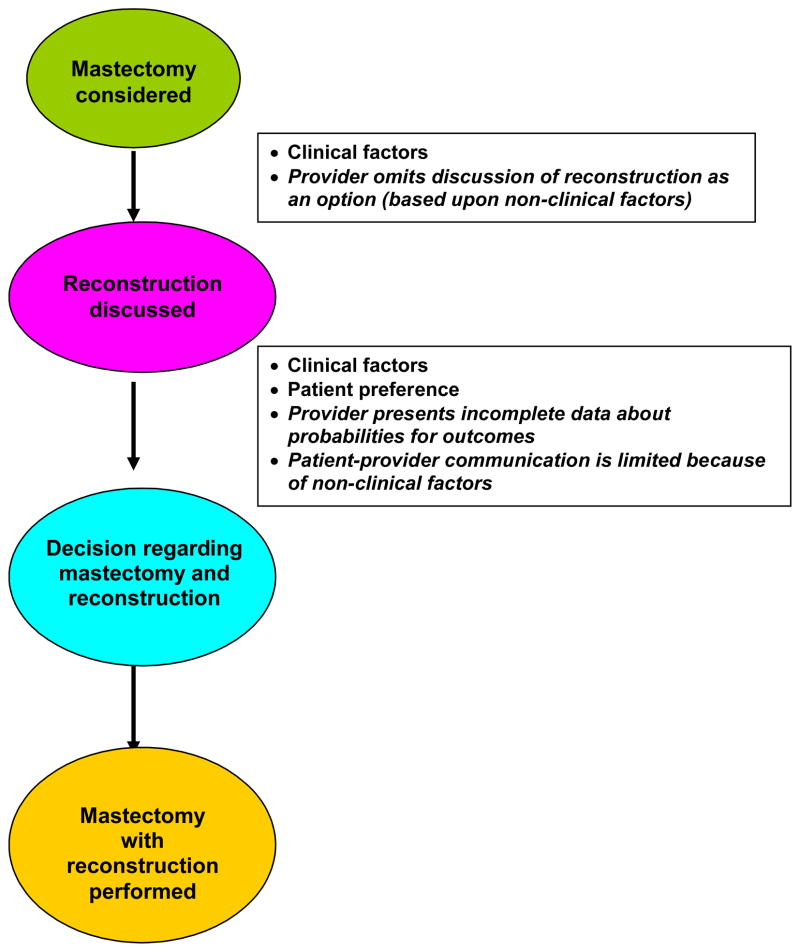
Background: The use of postmastectomy reconstruction varies with socioeconomic status, but the etiology of these variations is not understood. We investigated whether these differences reflect variations in the rate or qualitative aspects of the provider's discussion of reconstruction as an option.
Study design: Data were collected through chart review and patient survey for stages I to III breast cancer patients during the National Initiative on Cancer Care Quality. Multivariable logistic regression was used to identify predictors of reconstruction and discussion of reconstruction as an option. Predictors of not receiving reconstruction despite a documented discussion were also determined.
Results: There were 253 of 626 patients who received reconstruction (40.4%). Younger, more educated Caucasian women who were not overweight or receiving postmastectomy radiation were more likely to receive reconstruction. Patients who were younger, more educated, and not receiving postmastectomy radiation were more likely to have a documented discussion of reconstruction. If a discussion was documented, patients who were older, Hispanic, not born in the US, and received postmastectomy radiation were less likely to receive reconstruction. The greatest predictor of reconstruction was medical record documentation of a discussion about reconstruction.
Conclusions: We observed disparities in the likelihood of reconstruction that were at least partially explained by differences in the likelihood that reconstruction was discussed. But there were also differences in the likelihood of reconstruction based on age, race, and radiation once discussions occurred. Efforts to increase and improve discussions about reconstruction may decrease disparities for this procedure.
Conflict of interest statement
Competing Interests Declared: None.
Figures
Comment in
-
Invited commentary.J Am Coll Surg. 2012 Mar;214(3):276-9. doi: 10.1016/j.jamcollsurg.2011.12.021. J Am Coll Surg. 2012. PMID: 22365505 Free PMC article. No abstract available.
References
-
- Alderman AK, McMahon L, Jr, Wilkins EG. The national utilization of immediate and early delayed breast reconstruction and the effect of sociodemographic factors. Plast Reconstr Surg. 2003;111:695–703. discussion 704–705. - PubMed
-
- Desch CE, Penberthy LT, Hillner BE, et al. A sociodemographic and economic comparison of breast reconstruction, mastectomy, and conservative surgery. Surgery. 1999;125:441–447. - PubMed
-
- Hall SE, Holman CD. Inequalities in breast cancer reconstructive surgery according to social and locational status in Western Australia. Eur J Surg Oncol. 2003;29:519–525. - PubMed
-
- Morrow M, Scott SK, Menck HR, et al. Factors influencing the use of breast reconstruction postmastectomy: a National Cancer Database study. J Am Coll Surg. 2001;192:1–8. - PubMed
-
- Polednak AP. How frequent is postmastectomy breast reconstructive surgery? A study linking two statewide databases. Plast Reconstr Surg. 2001;108:73–77. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
