

Prevalence and evolution of intracranial hemorrhage in asymptomatic term infants
- PMID: 18388219
- PMCID: PMC8118856
- DOI: 10.3174/ajnr.A1004
Prevalence and evolution of intracranial hemorrhage in asymptomatic term infants
Abstract
Background and purpose: Subdural hemorrhage (SDH) is often associated with infants experiencing nonaccidental injury (NAI). A study of the appearance and natural evolution of these birth-related hemorrhages, particularly SDH, is important in the forensic evaluation of NAI. The purpose of this study was to determine the normal incidence, size, distribution, and natural history of SDH in asymptomatic term neonates as detected by sonography (US) and MR imaging within 72 hours of birth.
Materials and methods: Birth history, delivery method, duration of each stage of labor, pharmaceutic augmentation, and complications during delivery as well as postnatal physical examination were recorded. Brain MR imaging and US were performed on 101 asymptomatic term infants at 3-7 days, 2 weeks, 1 month, and 3 months. Clinical follow-up at 24 months was recorded.
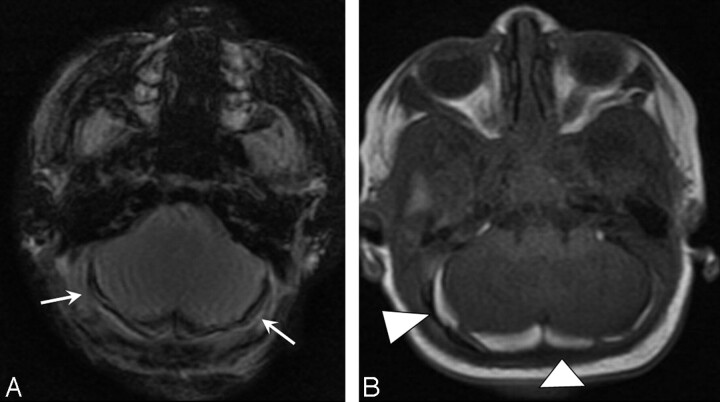
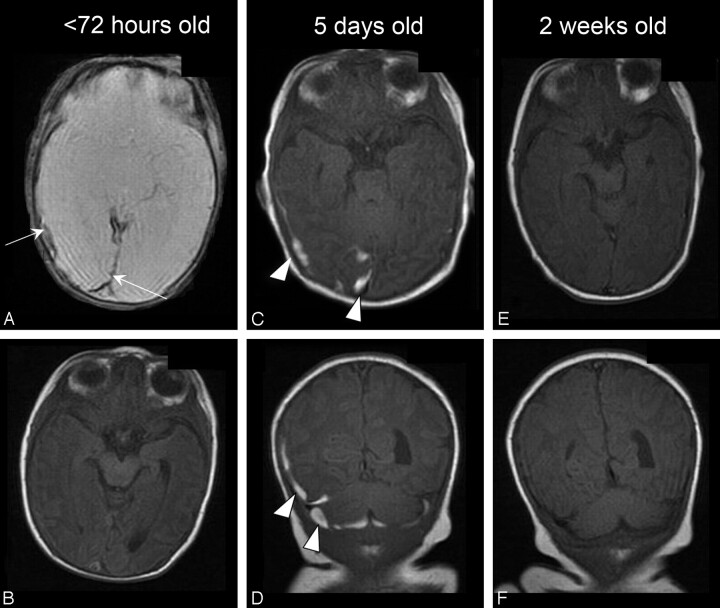
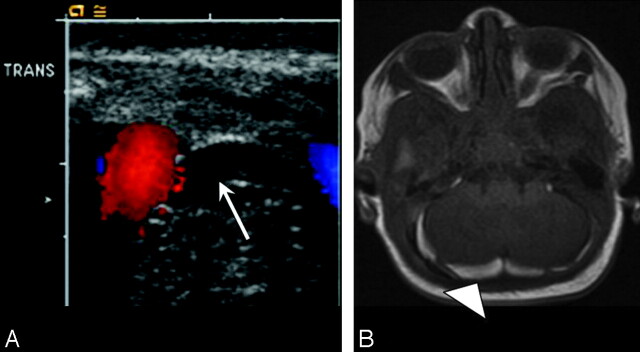
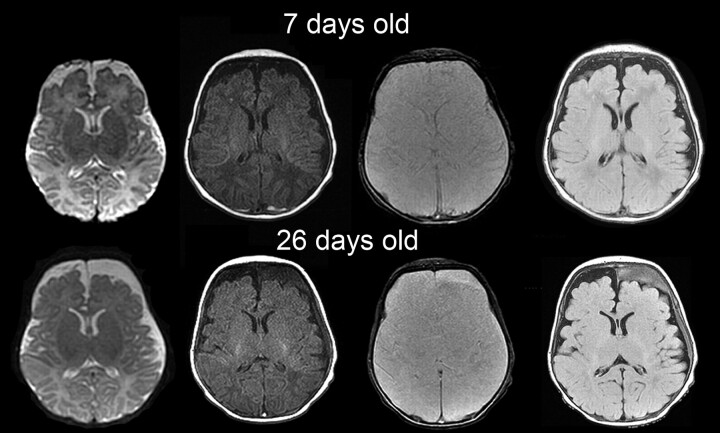
Results: Forty-six neonates had SDH by MR imaging within 72 hours of delivery. SDH was seen in both vaginal and cesarean deliveries. All neonates were asymptomatic, with normal findings on physical examination. All 46 had supratentorial SDH seen in the posterior cranium. Twenty (43%) also had infratentorial SDH. US detected 11 of the 20 (55%) infratentorial SDHs and no supratentorial SDH. Most SDHs present at birth were <or=3 mm and had resolved by 1 month, and all resolved by 3 months on MR imaging. Most children with SDHs had normal findings on developmental examinations at 24 months.
Conclusion: SDH in asymptomatic term neonates after delivery is limited in size and location.
Figures
Comment in
-
Is Delayed Speech Development a Long-Term Sequela of Birth-Related Subdural Hematoma?AJNR Am J Neuroradiol. 2019 Feb;40(2):E10. doi: 10.3174/ajnr.A5890. Epub 2019 Jan 24. AJNR Am J Neuroradiol. 2019. PMID: 30679223 Free PMC article. No abstract available.
References
-
- Barkovich AJ. Pediatric Neuroimaging. 3rd ed. New York: Lippincott Williams & Wilkins;2000
-
- Kleinman PK. Diagnostic Imaging of Child Abuse. 2nd ed. Toronto, Ontario, Canada: Mosby;1998
-
- Billmire ME, Myers PA. Serious head injury in infants: accident or abuse? Pediatrics 1985;75:340–42 - PubMed
-
- Hoskote A, Richards P, Anslow P, et al. Subdural haematoma and non-accidental head injury in children. Childs Nerv Syst 2002;18:311–17. Epub 2002 Jun 26 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical