

Endovascular coils as lung tumour markers in real-time tumour tracking stereotactic radiotherapy: preliminary results
- PMID: 18389249
- PMCID: PMC2469276
- DOI: 10.1007/s00330-008-0933-x
Endovascular coils as lung tumour markers in real-time tumour tracking stereotactic radiotherapy: preliminary results
Abstract
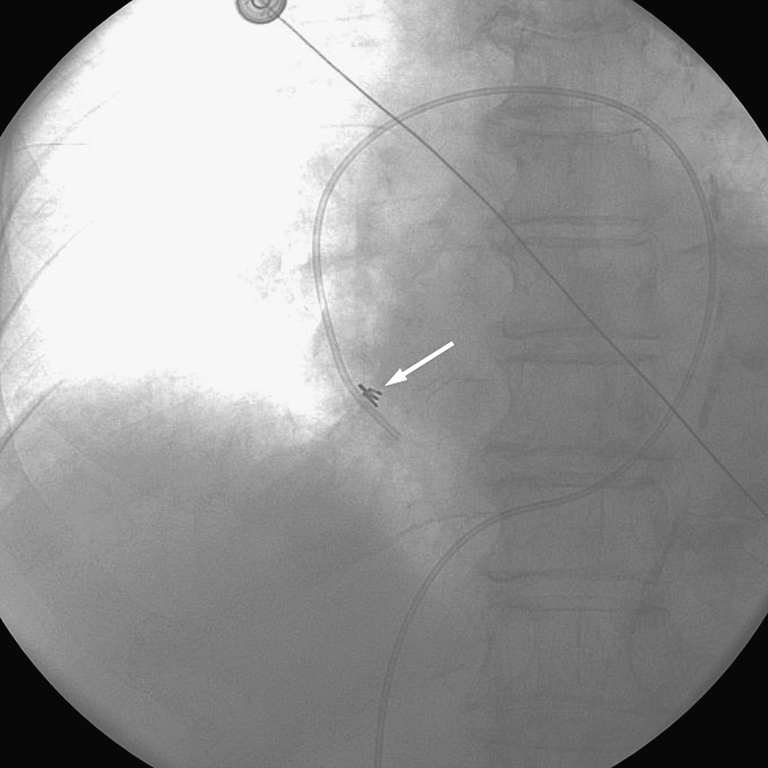
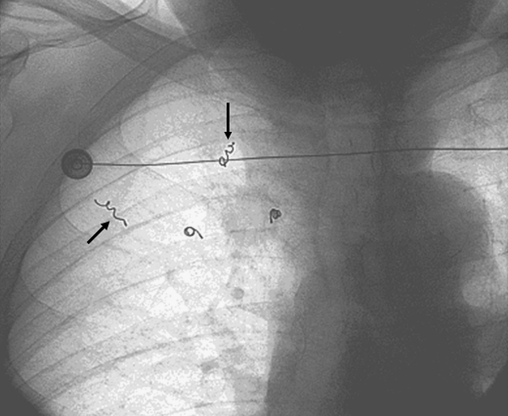
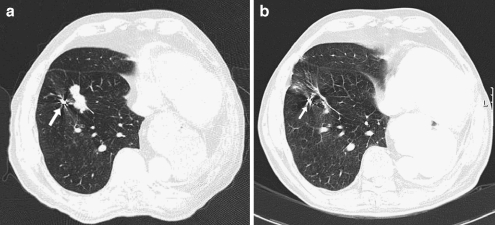
To evaluate the use of endovascular coils as markers for respiratory motion correction during high-dose stereotactic radiotherapy with the CyberKnife, an image-guided linear accelerator mounted on a robotic arm. Endovascular platinum embolisation coils were used to mark intrapulmonary lesions. The coils were placed in subsegmental pulmonary artery branches in close proximity to the target tumour. This procedure was attempted in 25 patients who were considered unsuitable candidates for standard transthoracic percutaneous insertion. Vascular coils (n = 87) were successfully inserted in 23 of 25 patients. Only minor complications were observed: haemoptysis during the procedure (one patient), development of pleural pain and fever on the day of procedure (one patient), and development of small infiltrative changes distal to the vascular coil (five patients). Fifty-seven coils (66% of total inserted number) could be used as tumour markers for delivery of biologically highly effective radiation doses with automated tracking during CyberKnife radiotherapy. Endovascular markers are safe and allow high-dose radiotherapy of lung tumours with CyberKnife, also in patients who are unsuitable candidates for standard transthoracic percutaneous marker insertion.
Figures

References
-
- Graham PH, Gebski VJ, Langlands AO. Radical radiotherapy for early nonsmall cell lung cancer. Int J Radiat Oncol Biol Phys. 1995;31:261–266. - PubMed
-
- Hanley J, Debois MM, Mah D. Deep inspiration breath hold technique for lung tumors: The potential value of target immobilization and reduced lung density in dose escalation. Int J Radiat Oncol Biol Phys. 1999;45:603–611. - PubMed
-
- Ohara K, Okumura T, Akisada M, et al. Irradiation synchronized with respiration gate. Int J Radiat Oncol Biol Phys. 1989;17:853–857. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
