

Examining asthma quality of care using a population-based approach
- PMID: 18390944
- PMCID: PMC2276554
- DOI: 10.1503/cmaj.070426
Examining asthma quality of care using a population-based approach
Abstract
Background: Asthma accounts for considerable burden on health care, but in most cases, asthma can be controlled. Quality-of-care indicators would aid in monitoring asthma management. We describe the quality of asthma care using a set of proposed quality indicators.
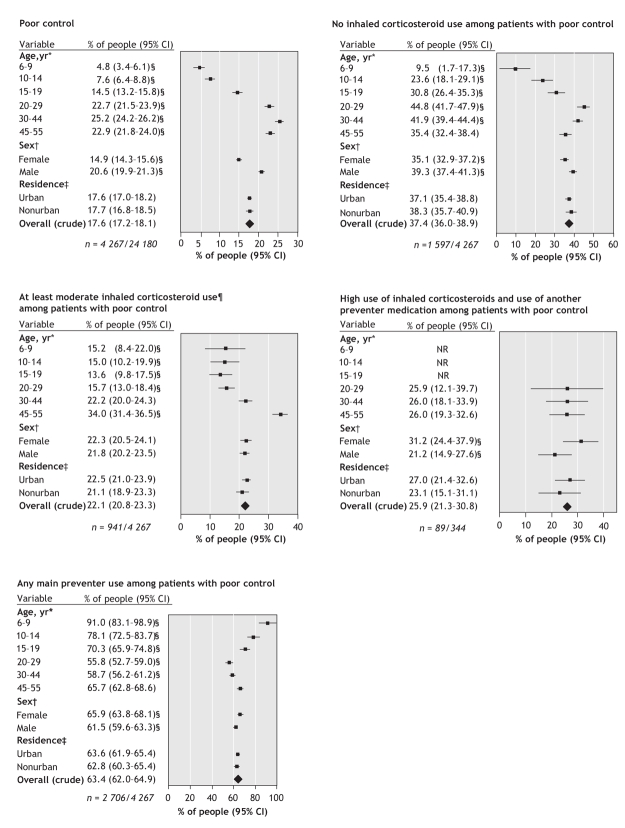
Methods: We performed a retrospective cross-sectional study using health databases in Saskatchewan, a Canadian province with a population of about 1 million people. We assessed 6 quality-of-care indicators among people with asthma: admission to hospital because of asthma; poor asthma control (high use of short-acting beta-agonists, admission to hospital because of asthma or death due to asthma); no inhaled corticosteroid use among patients with poor control; at least moderate inhaled corticosteroid use among patients with poor control; high inhaled corticosteroid use and use of another preventer medication among patients with poor control; and any main preventer use among patients with poor control. We calculated crude and adjusted rates with 95% confidence intervals. We tested for differences using the chi2 test for proportions and generalized linear modelling techniques.
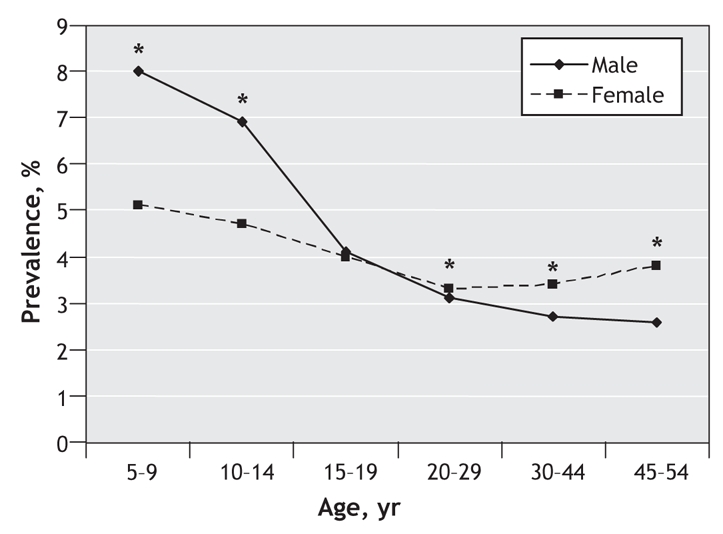
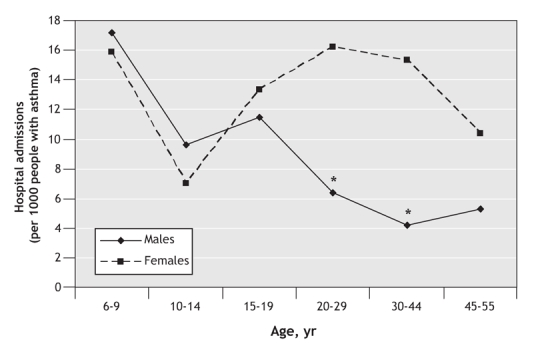
Results: In 2002/03, there were 24 616 people aged 5-54 years with asthma in Saskatchewan, representing a prevalence of 3.8%. Poor symptom control was observed in 18% of patients with asthma. Among those with poor control, 37% were not dispensed any inhaled corticosteroids, and 40% received potentially inadequate doses. Among those with poor control who were dispensed high doses of inhaled corticosteroids, 26% also used another preventer medication. Hospital admissions because of asthma were highest among those aged 6-9 years and females aged 20-44 years. Males and those in adult age groups (predominantly 20-44 years) had worse quality of care for 4 indicators examined.
Interpretation: Suboptimal asthma management would be improved through increased use of inhaled corticosteroids and preventer medications, and reduced reliance on short-acting beta-agonist medications as recommended by consensus guidelines.
Figures
Comment in
-
Asthma in Canada: missing the treatment targets.CMAJ. 2008 Apr 8;178(8):1027-8. doi: 10.1503/cmaj.080120. CMAJ. 2008. PMID: 18390947 Free PMC article. No abstract available.
References
-
- Canadian Institute for Health Information, Canadian Lung Association, Health Canada and Statistics Canada. Respiratory disease in Canada. Ottawa: The Institute; 2001. Available: www.phac-aspc.gc.ca/publicat/rdc-mrc01/index.html (accessed 2008 Jan 24).
-
- Mannino DM, Homa DM, Pertowski CA, et al. Surveillance for Asthma — United States, 1960–1995. MMWR CDC Surveill Summ 1998;47:1-27. - PubMed
-
- Senthilselvan A. Prevalence of physician-diagnosed asthma in Saskatchewan, 1981–1990. Chest 1998;114:388-92. - PubMed
-
- Glaxo Wellcome Inc. Asthma in Canada: a landmark survey. Mississauga (ON): Glaxo Wellcome Inc.; 2000.