

Elevated inflammation levels in depressed adults with a history of childhood maltreatment
- PMID: 18391129
- PMCID: PMC2923056
- DOI: 10.1001/archpsyc.65.4.409
Elevated inflammation levels in depressed adults with a history of childhood maltreatment
Erratum in
- Arch Gen Psychiatry. 2008 Jun;65(6):725
Abstract
Context: The association between depression and inflammation is inconsistent across research samples.
Objective: To test whether a history of childhood maltreatment could identify a subgroup of depressed individuals with elevated inflammation levels, thus helping to explain previous inconsistencies.
Design: Prospective longitudinal cohort study.
Setting: New Zealand.
Participants: A representative birth cohort of 1000 individuals was followed up to age 32 years as part of the Dunedin Multidisciplinary Health and Development Study. Study members were assessed for history of childhood maltreatment and current depression.
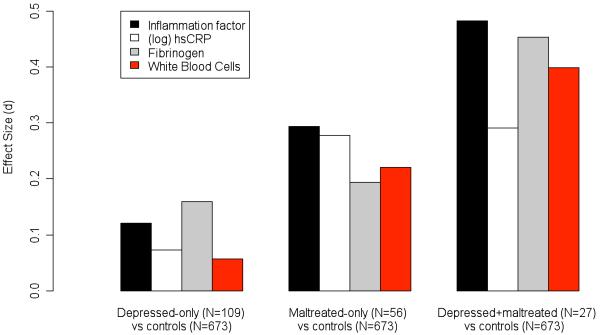
Main outcome measures: Inflammation was assessed using a clinically relevant categorical measure of high-sensitivity C-reactive protein (>3 mg/L) and a dimensional inflammation factor indexing the shared variance of continuous measures of high-sensitivity C-reactive protein, fibrinogen, and white blood cells.
Results: Although depression was associated with high levels of high-sensitivity C-reactive protein (relative risk,1.45; 95% confidence interval,1.06-1.99), this association was significantly attenuated and no longer significant when the effect of childhood maltreatment was taken into account. Individuals with current depression and a history of childhood maltreatment were more likely to have high levels of high-sensitivity C-reactive protein compared with control subjects (n = 27; relative risk, 2.07; 95% confidence interval, 1.23-3.47). In contrast, individuals with current depression only had a nonsignificant elevation in risk (n = 109; relative risk, 1.40; 95% confidence interval, 0.97-2.01). Results were generalizable to the inflammation factor. The elevated inflammation levels in individuals who were both depressed and maltreated were not explained by correlated risk factors such as depression recurrence, low socioeconomic status in childhood or adulthood, poor health, or smoking.
Conclusions: A history of childhood maltreatment contributes to the co-occurrence of depression and inflammation. Information about experiences of childhood maltreatment may help to identify depressed individuals with elevated inflammation levels and, thus, at greater risk of cardiovascular disease.
Figures
References
-
- Insel TR, Charney DS. Research on major depression: strategies and priorities. JAMA. 2003;289:3167–8. - PubMed
-
- Evans DL, Charney DS, Lewis L, Golden RN, Gorman JM, Krishnan KR, Nemeroff CB, Bremner JD, Carney RM, Coyne JC, Delong MR, Frasure-Smith N, Glassman AH, Gold PW, Grant I, Gwyther L, Ironson G, Johnson RL, Kanner AM, Katon WJ, Kaufmann PG, Keefe FJ, Ketter T, Laughren TP, Leserman J, Lyketsos CG, McDonald WM, McEwen BS, Miller AH, Musselman D, O’Connor C, Petitto JM, Pollock BG, Robinson RG, Roose SP, Rowland J, Sheline Y, Sheps DS, Simon G, Spiegel D, Stunkard A, Sunderland T, Tibbits P, Jr., Valvo WJ. Mood disorders in the medically ill: scientific review and recommendations. Biol Psychiatry. 2005;58:175–89. - PubMed
-
- Frasure-Smith N, Lesperance F, Talajic M. Depression following myocardial infarction. Impact on 6-month survival. JAMA. 1993;270:1819–25. - PubMed
-
- Berkman LF, Blumenthal J, Burg M, Carney RM, Catellier D, Cowan MJ, Czajkowski SM, DeBusk R, Hosking J, Jaffe A, Kaufmann PG, Mitchell P, Norman J, Powell LH, Raczynski JM, Schneiderman N. Effects of treating depression and low perceived social support on clinical events after myocardial infarction: the Enhancing Recovery in Coronary Heart Disease Patients (ENRICHD) Randomized Trial. JAMA. 2003;289:3106–16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
