

Achievement and maintenance of sustained response during the Treatment for Adolescents With Depression Study continuation and maintenance therapy
- PMID: 18391133
- PMCID: PMC2587406
- DOI: 10.1001/archpsyc.65.4.447
Achievement and maintenance of sustained response during the Treatment for Adolescents With Depression Study continuation and maintenance therapy
Abstract
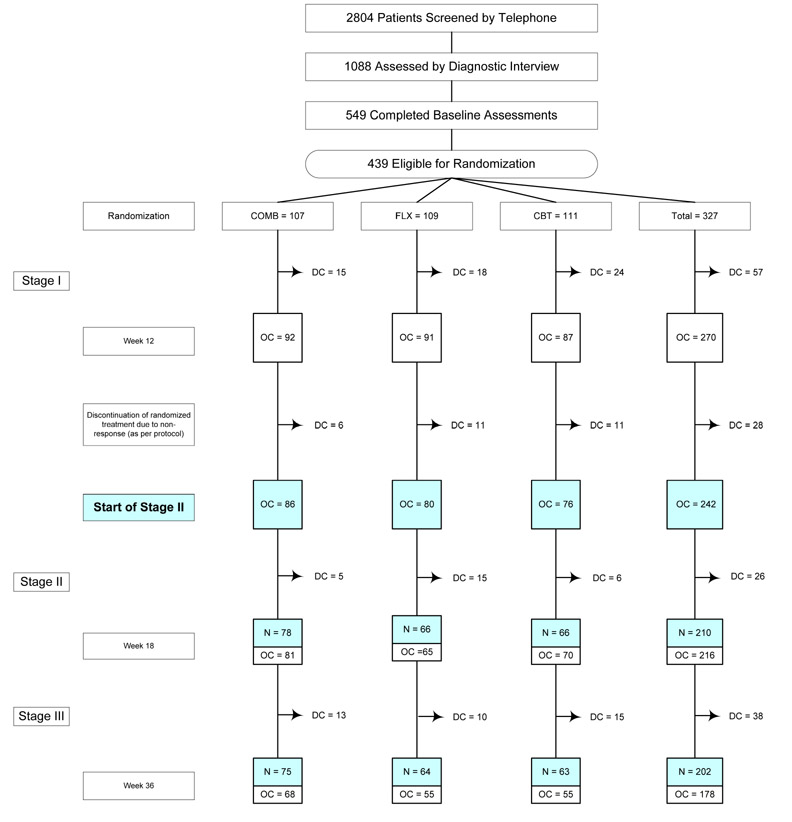
Context: The Treatment for Adolescents With Depression Study evaluated fluoxetine (FLX), cognitive behavioral therapy (CBT), and FLX/CBT combination (COMB) vs pill placebo in 439 adolescents with major depressive disorder. Treatment consisted of 3 stages: (1) acute (12 weeks), (2) continuation (6 weeks), and (3) maintenance (18 weeks).
Objective: To examine rates of achieving and maintaining sustained response during continuation and maintenance treatments.
Design: Randomized controlled trial. Response was determined by blinded independent evaluators.
Setting: Thirteen US sites.
Patients: Two hundred forty-two FLX, CBT, and COMB patients in their assigned treatment at the end of stage 1.
Interventions: Stage 2 treatment varied based on stage 1 response. Stage 3 consisted of 3 CBT and/or pharmacotherapy sessions and, if applicable, continued medication.
Main outcome measures: Sustained response was defined as 2 consecutive Clinical Global Impression-Improvement ratings of 1 or 2 ("full response"). Patients achieving sustained response were classified on subsequent nonresponse status.
Results: Among 95 patients (39.3%) who had not achieved sustained response by week 12 (29.1% COMB, 32.5% FLX, and 57.9% CBT), sustained response rates during stages 2 and 3 were 80.0% COMB, 61.5% FLX, and 77.3% CBT (difference not significant). Among the remaining 147 patients (60.7%) who achieved sustained response by week 12, CBT patients were more likely than FLX patients to maintain sustained response through week 36 (96.9% vs 74.1%; P = .007; 88.5% of COMB patients maintained sustained response through week 36). Total rates of sustained response by week 36 were 88.4% COMB, 82.5% FLX, and 75.0% CBT.
Conclusions: Most adolescents with depression who had not achieved sustained response during acute treatment did achieve that level of improvement during continuation and maintenance therapies. The possibility that CBT may help the subset of adolescents with depression who achieve early sustained response maintain their response warrants further investigation.
Trial registration: clinicaltrials.gov Identifier: NCT00006286.
Figures
References
-
- Mueller TI, Leon AD, Keller MG, Solomon DA, Endicott J, Coryell Y, Warshaw M, Maser JD. Recurrence after recovery from major depressive disorder during 15 years of observational follow-up. Am J Psychiatry. 1999;156:1000–1006. - PubMed
-
- Emslie GJ, Rush A, Weinberg W, Gullion D, Rintelmann J, Hughes C. Recurrence of major depressive disorder in hospitalized children and adolescents. J Am Acad Child Adoles Psychiatry. 1997;36:785–792. - PubMed
-
- Frank E, Prien RF, Jarrett RB, Keller MB, Kupfer DJ, Lavori PW, Rush AJ, Weissman MM. Conceptualization and rationale for consensus definitions of terms in major depressive disorder: Remission, recovery, relapse, and recurrence. Arch Gen Psychiatry. 1991;48:851–855. - PubMed
-
- Birmaher B, Brent D. Practice parameters for the assessment and treatment of children and adolescents with depressive disorders. J Am Acad Child Adolesc Psychiatry. 1998;37:63S–83S. - PubMed
-
- Park RJ, Goodyer IM. Clinical guidelines for depressive disorders in childhood and adolescence. Eur Child Adolesc Psychiatry. 2000;9:147–161. - PubMed
