

Principles of antegrade cerebral perfusion during arch reconstruction in newborns/infants
- PMID: 18396227
- PMCID: PMC2531241
- DOI: 10.1053/j.pcsu.2007.12.005
Principles of antegrade cerebral perfusion during arch reconstruction in newborns/infants
Abstract
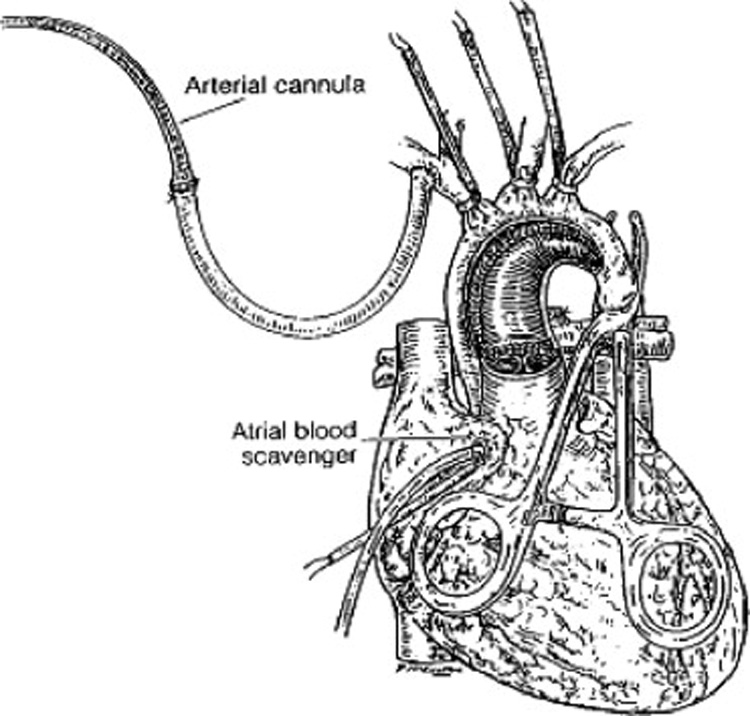
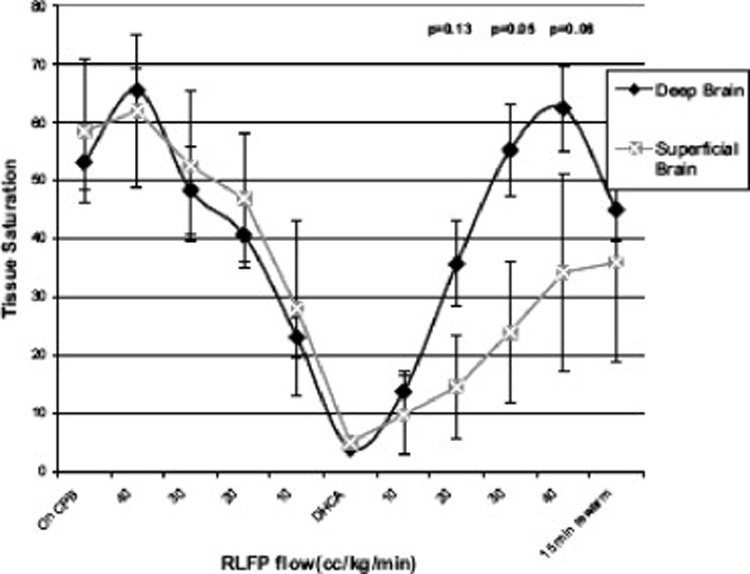
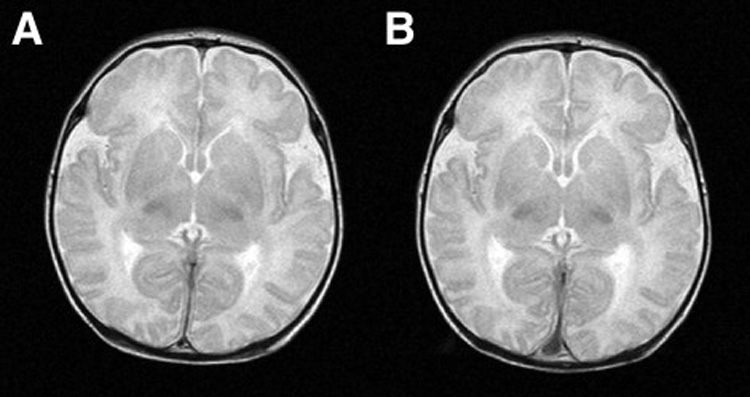
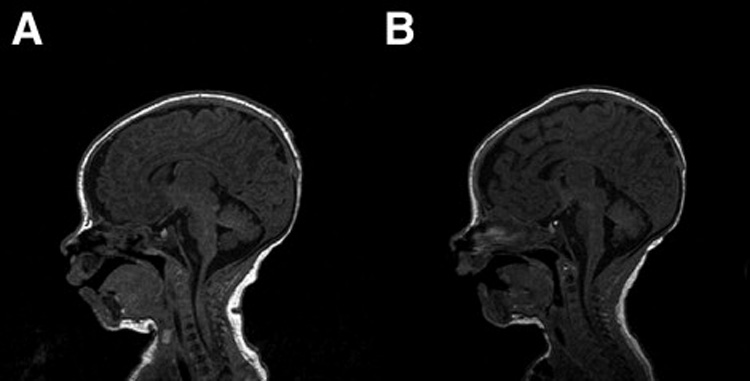
Antegrade cerebral perfusion (ACP) is a cardiopulmonary bypass technique that uses special cannulation procedures to perfuse only the brain during neonatal and infant aortic arch reconstruction. It is used in lieu of deep hypothermic circulatory arrest (DHCA), and thus has the theoretical advantage of protecting the brain from hypoxic ischemic injury. Despite this, recent comparative studies have shown no difference in neurodevelopmental outcomes with ACP versus DHCA for neonatal arch repair. This article presents animal and human data demonstrating that ACP flows less than 30 mL/kg/min are inadequate for many patients, and may be the explanation for lack of outcome difference versus DHCA. A technique for ACP, its physiologic basis, and a neuromonitoring strategy are presented, and then the results of an outcome study are reviewed, showing that with ACP technique at higher flows of 50 to 80 mL/kg/min guided by neuromonitoring, periventricular leukomalacia is eliminated on postoperative brain magnetic resonance imaging after neonatal cardiac surgery.
Figures
References
-
- Asou T, Kado H, Imoto Y, et al. Selective cerebral perfusion technique during aortic arch repair in neonates. Ann Thorac Surg. 1996;61:1546–1548. - PubMed
-
- Pigula FA, Nemoto EM, Siewers RD, Griffith BP. Regional perfusion of the brain during neonatal aortic arch reconstruction. J Thorac Cardiovasc Surg. 2000;117:1023–1024. - PubMed
-
- Pigula FA, Nemoto EM, Griffith BP, et al. Regional low-flow perfusion provides cerebral circulatory support during neonatal aortic arch reconstruction. J Thorac Cardiovasc Surg. 2000;119:331–339. - PubMed
-
- Wypij D, Newburger JW, Rappaport LA, et al. The effect of duration of deep hypothermic circulatory arrest in infant heart surgery on late neurodevelopment: the Boston Circulatory Arrest Trial. J Thorac Cardiovasc Surg. 2003;126:1397–1403. - PubMed
-
- Mahle WT, Cuadrado AR, Tam VK. Early experience with a modified Norwood procedure using right ventricle to pulmonary artery conduit. Ann Thorac Surg. 2003;76:1084–1088. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
