

The risk of extra-colonic, extra-endometrial cancer in the Lynch syndrome
- PMID: 18398828
- PMCID: PMC2627772
- DOI: 10.1002/ijc.23508
The risk of extra-colonic, extra-endometrial cancer in the Lynch syndrome
Abstract
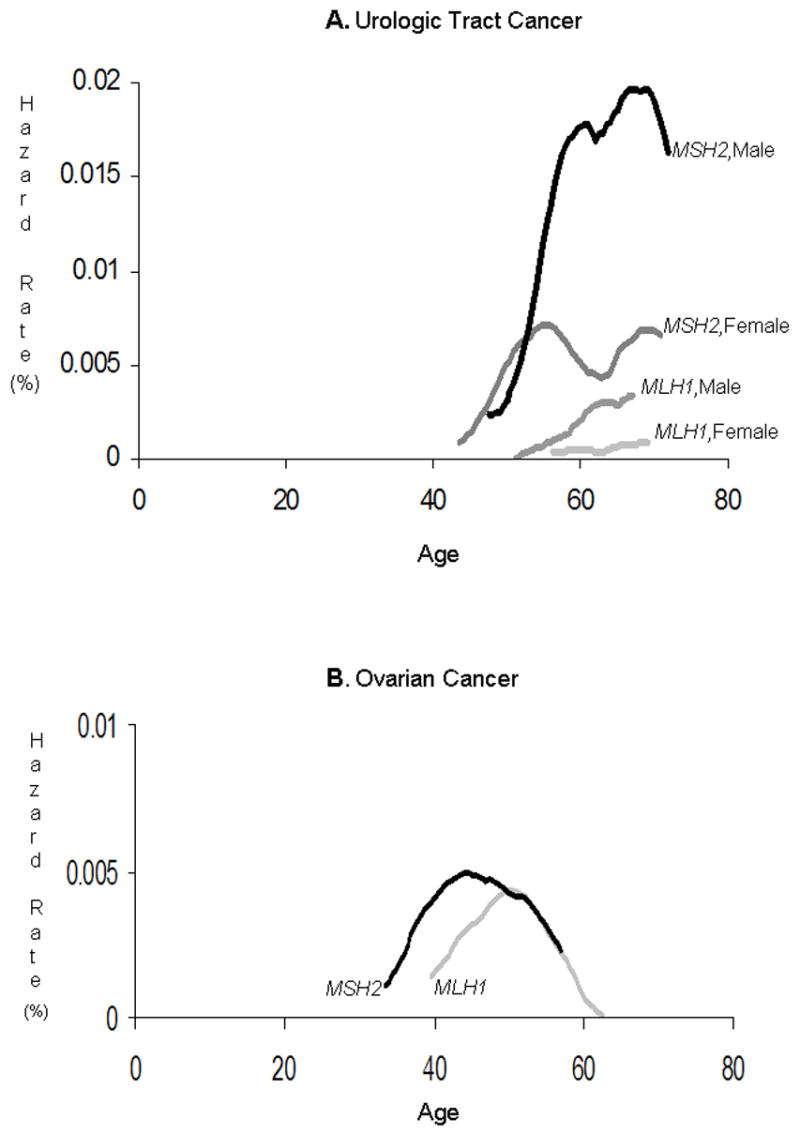
Persons with the Lynch syndrome (LS) are at high risk for cancer, including cancers of the small bowel, stomach, upper urologic tract (renal pelvis and ureter), ovary, biliary tract and brain tumors, in addition to the more commonly observed colorectal and endometrial cancers. Cancer prevention strategies for these less common cancers require accurate, age-specific risk estimation. We pooled data from 4 LS research centers in a retrospective cohort study, to produce absolute incidence estimates for these cancer types, and to evaluate several potential risk modifiers. After elimination of 135 persons missing crucial information, cohort included 6,041 members of 261 families with LS-associated MLH1 or MSH2 mutations. All were either mutation carriers by test, probable mutation carriers (endometrial/colorectal cancer-affected), or first-degree relatives of these. Among mutation carriers and probable carriers, urologic tract cancer (N = 98) had an overall lifetime risk (to age 70) of 8.4% (95% CI: 6.6-10.8); risks were higher in males (p < 0.02) and members of MSH2 families (p < 0.0001). Ovarian cancer (N = 72) had an lifetime risk of 6.7% (95% CI: 5.3-9.1); risks were higher in women born after the median year of birth (p < 0.008) and in members of MSH2 families (p < 0.006). Brain tumors and cancers of the small bowel, stomach, breast and biliary tract were less common. Urologic tract cancer and ovarian cancer occur frequently enough in some LS subgroups to justify trials to evaluate promising prevention interventions. Other cancer types studied occur too infrequently to justify strenuous cancer control interventions.
(c) 2008 Wiley-Liss, Inc.
Figures
References
-
- Watson P, Lynch HT. Extracolonic cancer in hereditary nonpolyposis colorectal cancer. Cancer. 1993;71:677–685. - PubMed
-
- Aarnio M, Sankila R, Pukkala E, Salovaara R, Aaltonen LA, de la Chapelle A, Peltomäki P, Mecklin J-P, Järvinen HJ. Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int J Cancer. 1999;81:214–218. - PubMed
-
- Boyd J, Rhei E, Federici MG, Borgen PI, Watson P, Franklin B, Karr B, Lynch J, Lemon SJ, Lynch HT. Male breast cancer in the hereditary nonpolyposis colorectal cancer syndrome. Breast Cancer Res Treat. 1999;53:87–91. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
