

Long-term interleukin-6 levels and subsequent risk of coronary heart disease: two new prospective studies and a systematic review
- PMID: 18399716
- PMCID: PMC2288623
- DOI: 10.1371/journal.pmed.0050078
Long-term interleukin-6 levels and subsequent risk of coronary heart disease: two new prospective studies and a systematic review
Abstract
Background: The relevance to coronary heart disease (CHD) of cytokines that govern inflammatory cascades, such as interleukin-6 (IL-6), may be underestimated because such mediators are short acting and prone to fluctuations. We evaluated associations of long-term circulating IL-6 levels with CHD risk (defined as nonfatal myocardial infarction [MI] or fatal CHD) in two population-based cohorts, involving serial measurements to enable correction for within-person variability. We updated a systematic review to put the new findings in context.
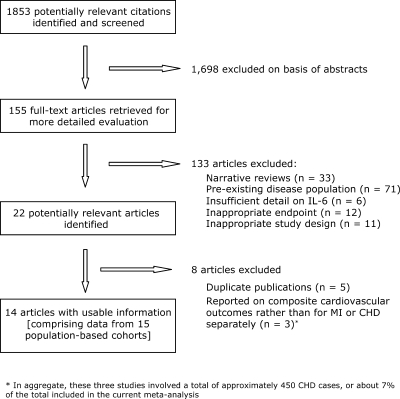
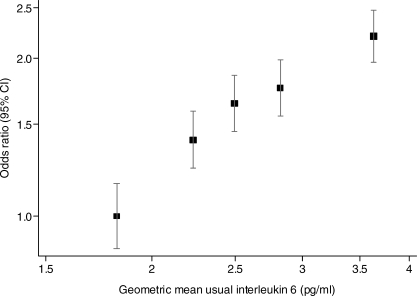
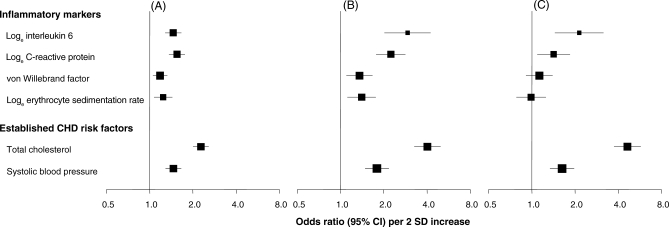
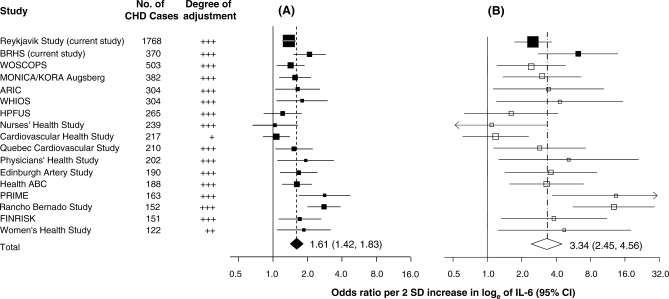
Methods and findings: Measurements were made in samples obtained at baseline from 2,138 patients who had a first-ever nonfatal MI or died of CHD during follow-up, and from 4,267 controls in two cohorts comprising 24,230 participants. Correction for within-person variability was made using data from repeat measurements taken several years apart in several hundred participants. The year-to-year variability of IL-6 values within individuals was relatively high (regression dilution ratios of 0.41, 95% confidence interval [CI] 0.28-0.53, over 4 y, and 0.35, 95% CI 0.23-0.48, over 12 y). Ignoring this variability, we found an odds ratio for CHD, adjusted for several established risk factors, of 1.46 (95% CI 1.29-1.65) per 2 standard deviation (SD) increase of baseline IL-6 values, similar to that for baseline C-reactive protein. After correction for within-person variability, the odds ratio for CHD was 2.14 (95% CI 1.45-3.15) with long-term average ("usual") IL-6, similar to those for some established risk factors. Increasing IL-6 levels were associated with progressively increasing CHD risk. An updated systematic review of electronic databases and other sources identified 15 relevant previous population-based prospective studies of IL-6 and clinical coronary outcomes (i.e., MI or coronary death). Including the two current studies, the 17 available prospective studies gave a combined odds ratio of 1.61 (95% CI 1.42-1.83) per 2 SD increase in baseline IL-6 (corresponding to an odds ratio of 3.34 [95% CI 2.45-4.56] per 2 SD increase in usual [long-term average] IL-6 levels).
Conclusions: Long-term IL-6 levels are associated with CHD risk about as strongly as are some major established risk factors, but causality remains uncertain. These findings highlight the potential relevance of IL-6-mediated pathways to CHD.
Conflict of interest statement
Figures
References
-
- Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352:1685–1695. - PubMed
-
- Pearson TA, Mensah GA, Alexander RW, Anderson JL, Cannon RO, III, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the Centers for Disease Control and Prevention and the American Heart Association. Circulation. 2003;107:499–511. - PubMed
-
- Kerr R, Stirling D, Ludlam CA. Interleukin 6 and haemostasis. Br J Haematol. 2001;115:3–12. - PubMed
-
- Le JM, Vilcek J. Interleukin 6: a multifunctional cytokine regulating immune reactions and the acute phase protein response. Lab Invest. 1989;61:588–602. - PubMed
-
- Woodward M, Rumley A, Tunstall-Pedoe H, Lowe GD. Associations of blood rheology and interleukin-6 with cardiovascular risk factors and prevalent cardiovascular disease. Br J Haematol. 1999;104:246–257. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
