

New aspects of neotropical polycystic (Echinococcus vogeli) and unicystic (Echinococcus oligarthrus) echinococcosis
- PMID: 18400802
- PMCID: PMC2292577
- DOI: 10.1128/CMR.00050-07
New aspects of neotropical polycystic (Echinococcus vogeli) and unicystic (Echinococcus oligarthrus) echinococcosis
Abstract
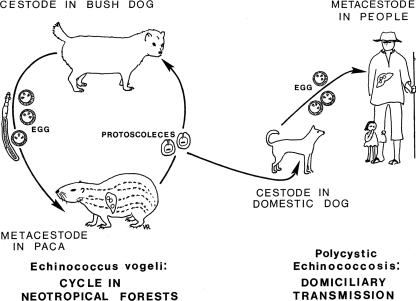
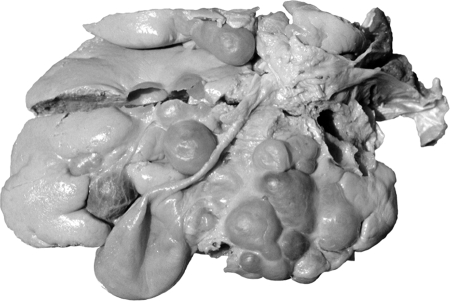
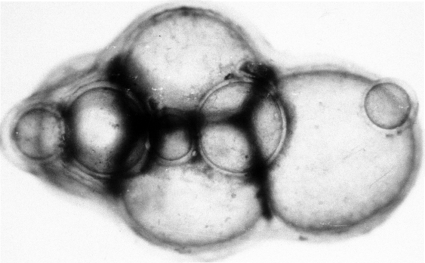
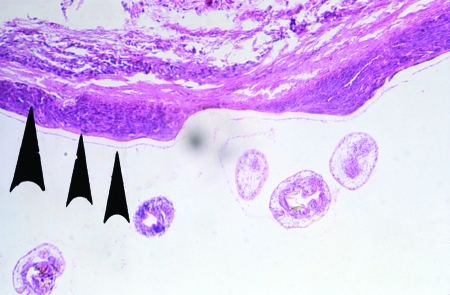
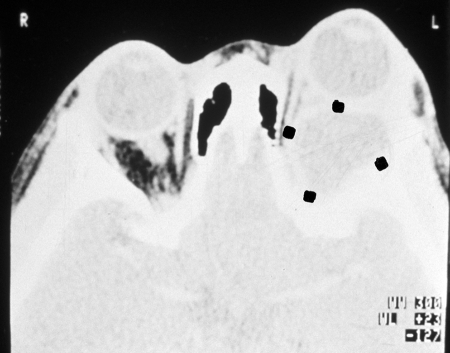
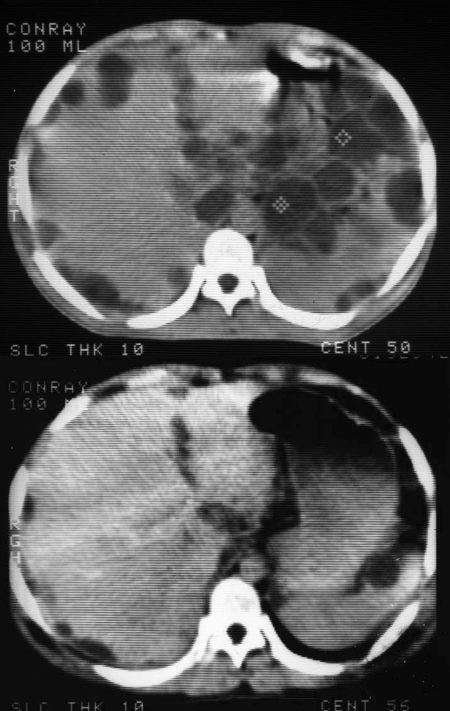
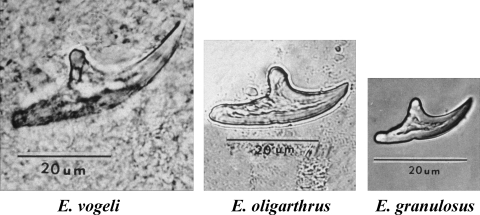
Of the four species of the genus Echinococcus (Cestoda) distinguished by biological and morphological characteristics, two species, E. vogeli and E. oligarthrus, occur widely in the Neotropics. Approximately 200 cases of polycystic echinococcosis (PE) have been recorded from 12 countries in South America. Following early proliferation of E. vogeli in the human host, typically in the liver, the metacestode usually spreads in the peritoneal and pleural cavities, and numerous organs may be invaded. The clinical characteristics of PE in 81 patients with sufficient information are reviewed. Type I disease consists of polycysts in the liver and abdominal cavity (37% of the patients had this characteristic); type II is similar to type I but also includes hepatic insufficiency (26%); type III consists of cysts in liver and chest (14%); type IV consists of cysts only in the mesenteries (16%); and type V consists of cysts calcified in liver and lung (4%). The percentage of patients with polycysts in the liver was 81%, and the percentage of patients with polycysts in the chest was 14%. PE is most ready diagnosed by geographic origin of the patient and by means of ultrasound or computerized tomography scanning showing cysts and calcifications. The highest mortality was for patients with type II disease, due to hepatic failure and its complications. There were five patients who died due to surgical accidents, whereas 35 cases had uncomplicated surgery. Twenty-three patients died of PE, making the total mortality 29% (23 of 78 cases). None of the 13 patients treated only with albendazole, the most efficacious treatment, was completely cured. PE represents a severe medical problem in South America. A reevaluation of the characteristics of the metacestode of E. oligarthrus indicated that it is unicystic. Only three human cases are known (two with infection in the orbit and one with infection in the heart). The metacestode of E. oligarthrus, in contrast with that of E. vogeli, consists of a spherical, fluid-filled vesicle that enlarges concentrically and is not known to undergo exogenous proliferation.
Figures
















Similar articles
-
Neotropical echinococcosis in Suriname: Echinococcus oligarthrus in the orbit and Echinococcus vogeli in the abdomen.Am J Trop Med Hyg. 1998 Nov;59(5):787-90. doi: 10.4269/ajtmh.1998.59.787. Am J Trop Med Hyg. 1998. PMID: 9840599
-
Polycystic echinococcosis in tropical America: Echinococcus vogeli and E. oligarthrus.Acta Trop. 1997 Sep 15;67(1-2):43-65. doi: 10.1016/s0001-706x(97)00048-x. Acta Trop. 1997. PMID: 9236939 Review.
-
Echinococcus vogeli in man, with a review of polycystic hydatid disease in Colombia and neighboring countries.Am J Trop Med Hyg. 1979 Mar;28(2):303-17. doi: 10.4269/ajtmh.1979.28.303. Am J Trop Med Hyg. 1979. PMID: 572148
-
Polycystic hydatid disease (Echinococcus vogeli). Clinical, laboratory and morphological findings in nine Brazilian patients.J Hepatol. 1992 Mar;14(2-3):203-10. doi: 10.1016/0168-8278(92)90159-m. J Hepatol. 1992. PMID: 1500684
-
Phylogenetic systematics of the genus Echinococcus (Cestoda: Taeniidae).Int J Parasitol. 2013 Nov;43(12-13):1017-29. doi: 10.1016/j.ijpara.2013.06.002. Epub 2013 Jul 18. Int J Parasitol. 2013. PMID: 23872521 Review.
Cited by
-
Epidemiological studies on Echinococcus in Pampas fox (Lycalopex gymnocercus) and European hare (Lepus europaeus) in Buenos Aires province, Argentina.Parasitol Res. 2013 Oct;112(10):3607-13. doi: 10.1007/s00436-013-3548-3. Epub 2013 Jul 28. Parasitol Res. 2013. PMID: 23892482
-
A rare presentation of hydatid cyst in abdominal wall: case report.Pan Afr Med J. 2021 Dec 21;40:246. doi: 10.11604/pamj.2021.40.246.32301. eCollection 2021. Pan Afr Med J. 2021. PMID: 35233266 Free PMC article.
-
Update of Cestodes Parasitizing Neotropical Hystricomorphic Rodent.Front Vet Sci. 2022 Apr 29;9:885678. doi: 10.3389/fvets.2022.885678. eCollection 2022. Front Vet Sci. 2022. PMID: 35573400 Free PMC article. Review.
-
Effect of sunitinib against Echinococcus multilocularis through inhibition of VEGFA-induced angiogenesis.Parasit Vectors. 2023 Nov 7;16(1):407. doi: 10.1186/s13071-023-05999-4. Parasit Vectors. 2023. PMID: 37936208 Free PMC article.
-
Zoonotic helminths affecting the human eye.Parasit Vectors. 2011 Mar 23;4:41. doi: 10.1186/1756-3305-4-41. Parasit Vectors. 2011. PMID: 21429191 Free PMC article. Review.
References
-
- Abuladze, K. I. 1964. Teniaty—lentochnye gel'minty zhivotnykh i cheloveka i vyzyvaemye imi zabolevaniia. Osnovy tsestodologii, vol. 4. Nauka, Moskva, U.S.S.R.
-
- Almeida, S. C. X., R. L. Martins, A. P. Morales, C. A. Viegas, and M. Grilo. 1997. Hidatidosis pulmonar policística mimetizando lesaôs metastáticas: relato de caso. J. Pneumonol. 23:261-263.
-
- Alvarez, V. 1961. Investigaciones sobre echinococcosis silvestre en Chile. Biologica 31:89-94. - PubMed
-
- Basset, D., C. Girou, I. P. Nozais, F. D'Hermies, C. Hoang, R. Gordon, and A. D'Alessandro. 1998. Neotropical echinococcosis in Suriname: Echinococcus oligarthrus in the orbit and Echinococcus vogeli in the abdomen. Am. J. Trop. Med. Hyg. 59:787-790. - PubMed
-
- Blood, B. D., and J. L. Lelijveld. 1969. Studies on sylvatic echinococcosis in southern South America. Z. Tropenmed. Parasitol. 20:475-482. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
