

Pitfalls of measuring total blood calcium in patients with CKD
- PMID: 18400941
- PMCID: PMC2488254
- DOI: 10.1681/ASN.2007040449
Pitfalls of measuring total blood calcium in patients with CKD
Abstract
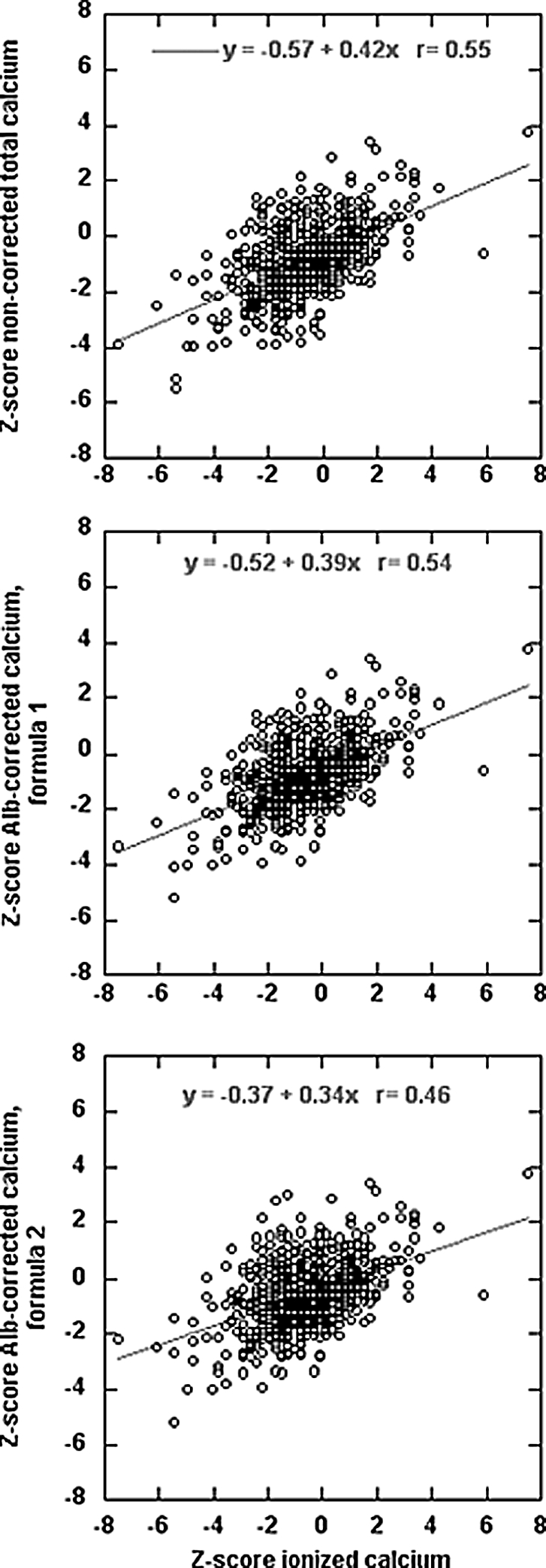
Disorders of mineral and bone metabolism are prevalent in patients with chronic kidney disease (CKD). The recent National Kidney Foundation Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines recommend that blood calcium (Ca) be regularly measured in patients with stages 3 to 5 CKD. The Kidney Disease: Improving Global Outcomes (KDIGO) position states that the measurement of ionized Ca (iCa) is preferred and that if total Ca (tCa) concentration is used instead, then it should be adjusted in the setting of hypoalbuminemia. In 691 consecutive patients with stages 3 to 5 CKD, we compared the ability of noncorrected and albumin-corrected tCa concentration to identify low, normal, or high iCa concentration. The agreement between noncorrected or albumin-corrected tCa and iCa was only fair. The risk for underestimating ionized calcium was independently increased by a low total CO(2) concentration when either noncorrected or albumin-corrected Ca was used and by a low albumin concentration only when noncorrected tCa was used. The risk for overestimating iCa was increased by a low albumin concentration only when albumin-corrected Ca was used. In conclusion, albumin-corrected tCa does not predict iCa better than noncorrected tCa. Moreover, both noncorrected and albumin-corrected tCa concentrations poorly predict hypo- or hypercalcemia in patients with CKD.
Figures
References
-
- Block GA, Klassen PS, Lazarus JM, Ofsthun N, Lowrie EG, Chertow GM: Mineral metabolism, mortality, and morbidity in maintenance hemodialysis. J Am Soc Nephrol 15: 2208–2218, 2004 - PubMed
-
- Young EW, Albert JM, Satayathum S, Goodkin DA, Pisoni RL, Akiba T, Akizawa T, Kurokawa K, Bommer J, Piera L, Port FK: Predictors and consequences of altered mineral metabolism: The Dialysis Outcomes and Practice Patterns Study. Kidney Int 67: 1179–1187, 2005 - PubMed
-
- K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 42: S1–201, 2003 - PubMed
-
- Moe S, Drueke T, Cunningham J, Goodman W, Martin K, Olgaard K, Ott S, Sprague S, Lameire N, Eknoyan G: Definition, evaluation, and classification of renal osteodystrophy: A position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 69: 1945–1953, 2006 - PubMed
-
- Boink AB, Buckley BM, Christiansen TF, Covington AK, Maas AH, Muller-Plathe O, Sachs C, Siggaard-Andersen O: Recommendation on sampling, transport, and storage for the determination of the concentration of ionized calcium in whole blood, plasma, and serum. IFC Scientific Division, Working Group on Ion-Selective Electrodes (WGSE). J Int Fed Clin Chem 4: 147–152, 1992 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
