

Effects of arterial stiffness, pulse wave velocity, and wave reflections on the central aortic pressure waveform
- PMID: 18401227
- PMCID: PMC8110097
- DOI: 10.1111/j.1751-7176.2008.04746.x
Effects of arterial stiffness, pulse wave velocity, and wave reflections on the central aortic pressure waveform
Abstract
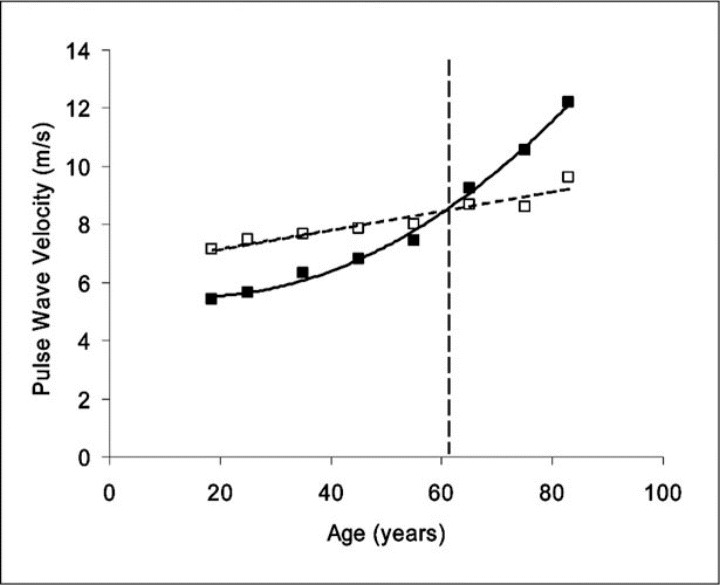
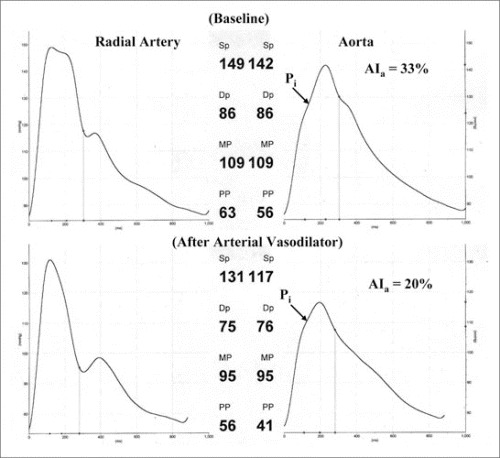
Brachial systolic and pulse blood pressures (BPs) are better predictors of adverse cardiovascular (CV) events than diastolic BP in individuals older than 50 years. The principal cause of increased systolic and pulse BP is increased stiffness of the elastic arteries as a result of degeneration and hyperplasia of the arterial wall. Recent studies have shown that central BP, the pressure exerted on the heart, brain, and kidneys, is a better predictor of CV risk than brachial BP. As stiffness increases, reflected wave amplitude increases and augments pressure in late systole, producing an increase in left ventricular afterload and myocardial oxygen demand. Vasoactive drugs have little direct effect on large human elastic arteries but can markedly modify wave reflection by altering stiffness of the muscular arteries and changing pulse wave velocity of the reflected wave from the periphery to the heart. Vasodilators decrease the amplitude and increase the travel time (or delay) of the reflected wave, causing a generalized decrease in systolic BP. The decrease in systolic BP brought about by this mechanism is grossly underestimated when systolic BP is measured in the brachial artery.
Figures


Similar articles
-
Arterial elastance and wave reflection augmentation of systolic blood pressure: deleterious effects and implications for therapy.J Cardiovasc Pharmacol Ther. 2001 Jan;6(1):5-21. doi: 10.1177/107424840100600102. J Cardiovasc Pharmacol Ther. 2001. PMID: 11452332 Review.
-
Clinical measurement of arterial stiffness obtained from noninvasive pressure waveforms.Am J Hypertens. 2005 Jan;18(1 Pt 2):3S-10S. doi: 10.1016/j.amjhyper.2004.10.009. Am J Hypertens. 2005. PMID: 15683725 Review.
-
Arterial stiffness, systolic blood pressure, and logical treatment of arterial hypertension.Hypertension. 1990 Apr;15(4):339-47. doi: 10.1161/01.hyp.15.4.339. Hypertension. 1990. PMID: 2180816 Review.
-
Augmentation index as a measure of peripheral vascular disease state.Curr Opin Cardiol. 2002 Sep;17(5):543-51. doi: 10.1097/00001573-200209000-00016. Curr Opin Cardiol. 2002. PMID: 12357133 Review.
-
Actions of selected cardiovascular hormones on arterial stiffness and wave reflections.Curr Pharm Des. 2009;15(3):304-20. doi: 10.2174/138161209787354258. Curr Pharm Des. 2009. PMID: 19149620 Review.
Cited by
-
Ventricular-arterial coupling: Invasive and non-invasive assessment.Artery Res. 2013 Mar;7(1):10.1016/j.artres.2012.12.002. doi: 10.1016/j.artres.2012.12.002. Artery Res. 2013. PMID: 24179554 Free PMC article.
-
Association of plasma B-type natriuretic peptide concentrations with longitudinal blood pressure tracking in African Americans: findings from the Jackson Heart Study.Hypertension. 2013 Jan;61(1):48-54. doi: 10.1161/HYPERTENSIONAHA.112.197657. Epub 2012 Nov 26. Hypertension. 2013. PMID: 23184379 Free PMC article.
-
Patient-Specific Haemodynamic Analysis of Virtual Grafting Strategies in Type-B Aortic Dissection: Impact of Compliance Mismatch.Cardiovasc Eng Technol. 2024 Jun;15(3):290-304. doi: 10.1007/s13239-024-00713-6. Epub 2024 Mar 4. Cardiovasc Eng Technol. 2024. PMID: 38438692 Free PMC article.
-
Battery-free, stretchable optoelectronic systems for wireless optical characterization of the skin.Sci Adv. 2016 Aug 3;2(8):e1600418. doi: 10.1126/sciadv.1600418. eCollection 2016 Aug. Sci Adv. 2016. PMID: 27493994 Free PMC article.
-
Effect of whole-body mild-cold exposure on arterial stiffness and central haemodynamics: a randomised, cross-over trial in healthy men and women.Eur J Appl Physiol. 2013 May;113(5):1257-69. doi: 10.1007/s00421-012-2543-1. Epub 2012 Nov 18. Eur J Appl Physiol. 2013. PMID: 23160656 Clinical Trial.
References
-
- The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003;289(19):2560–2572. - PubMed
-
- Haider AW, Larson MG, Franklin SS, et al. Systolic blood pressure, diastolic blood pressure, and pulse pressure as predictors of risk for congestive heart failure in the Framingham Heart Study. Ann Intern Med. 2003;138(1):10–16. - PubMed
-
- Lewington S, Clarke R, Qizilbash N, et al. Age‐specific relevance of usual blood pressure to vascular mortality: a meta‐analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360(9349):1903–1913. - PubMed
-
- Chirinos JA, Zambrano JP, Chakko S, et al. Relation between ascending aortic pressures and outcomes in patients with angiographically demonstrated coronary artery disease. Am J Cardiol. 2005;96(5):645–648. - PubMed
-
- Nichols WW, O'Rourke MF. McDonald's Blood Flow in Arteries: Theoretic, Experimental and Clinical Principles. 5th ed. London, England: Edward Arnold; 2005.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
