

Clinical validation of percutaneous cochlear implant surgery: initial report
- PMID: 18401279
- PMCID: PMC4453765
- DOI: 10.1097/MLG.0b013e31816b309e
Clinical validation of percutaneous cochlear implant surgery: initial report
Abstract
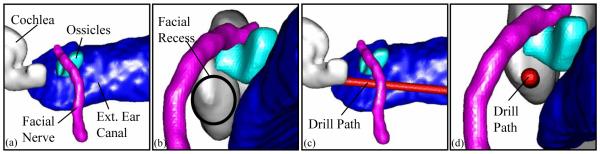
Objective: Percutaneous cochlear implant surgery consists of a single drill path from the lateral mastoid cortex to the cochlea via the facial recess. We sought to clinically validate this technique in patients undergoing traditional cochlear implant surgery.
Study design: Prospective clinical trial.
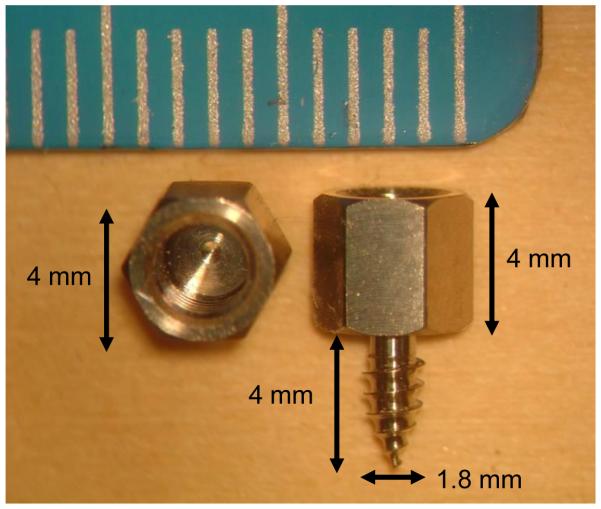
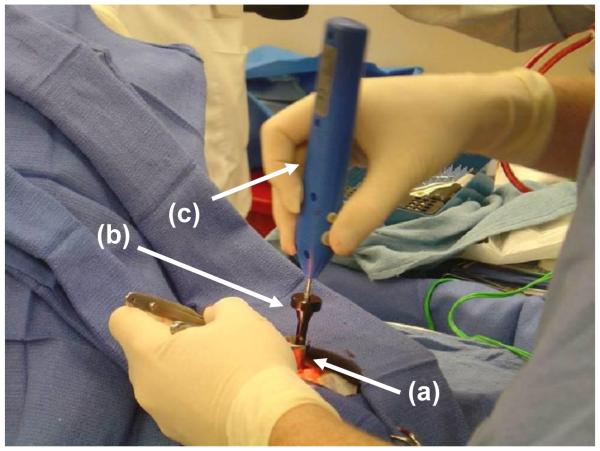
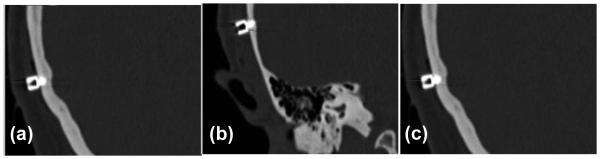
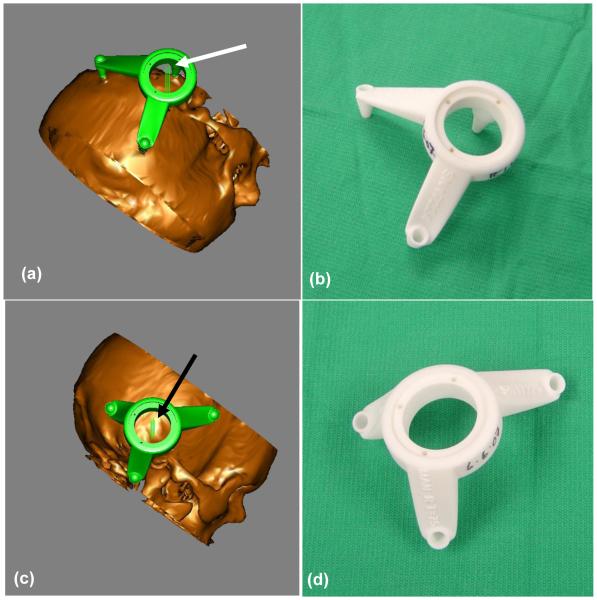
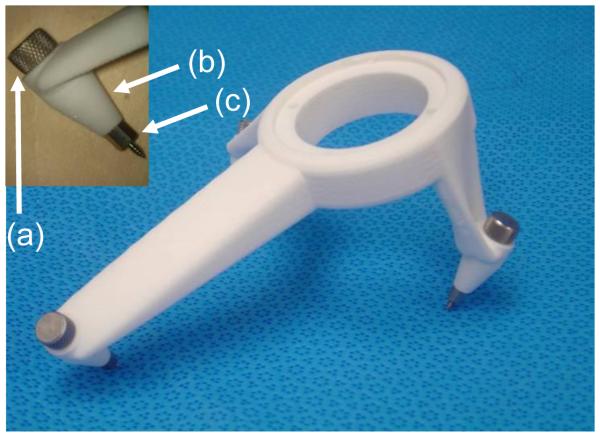
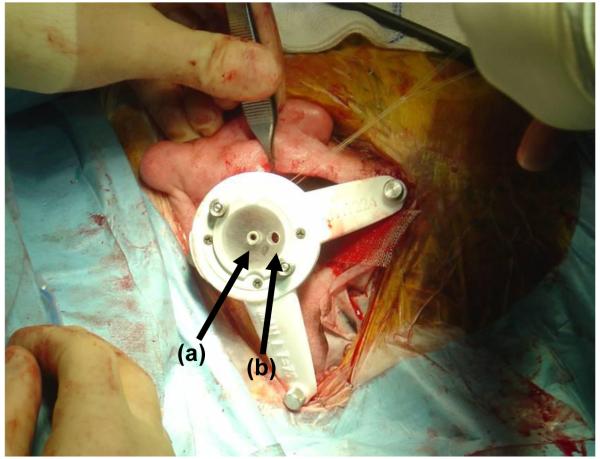
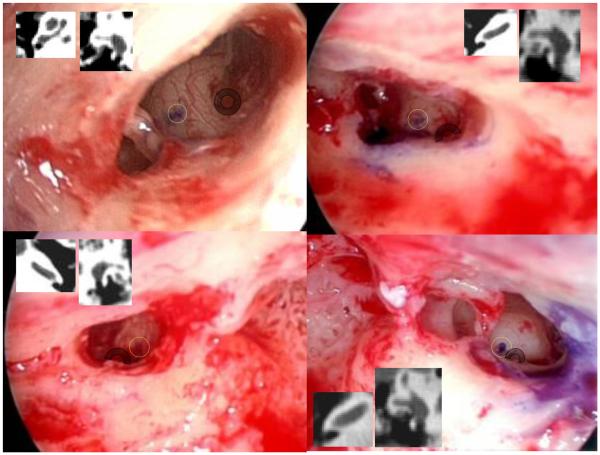
Methods: After institutional regulatory board-approved protocols, five ears were studied via the following steps. 1) In the clinic under local anesthesia, bone-implanted anchors were placed surrounding each mastoid. 2) Temporal-bone computed tomography (CT) scans were obtained. 3) On the CT scans, paths were planned from the lateral mastoid cortex, through the facial recess, to the basal turn of the cochlea both "manually" and "automatically" using computer software. 4) Customized microstereotactic frames were rapid-prototyped to serve as drill guides constraining the drill to follow the appropriate path. 5) During cochlear implant surgery, after drilling of the facial recess, drill guides were mounted on the bone-implanted anchors. 6) Accuracy of paths was assessed via intraoperative photodocumentation.
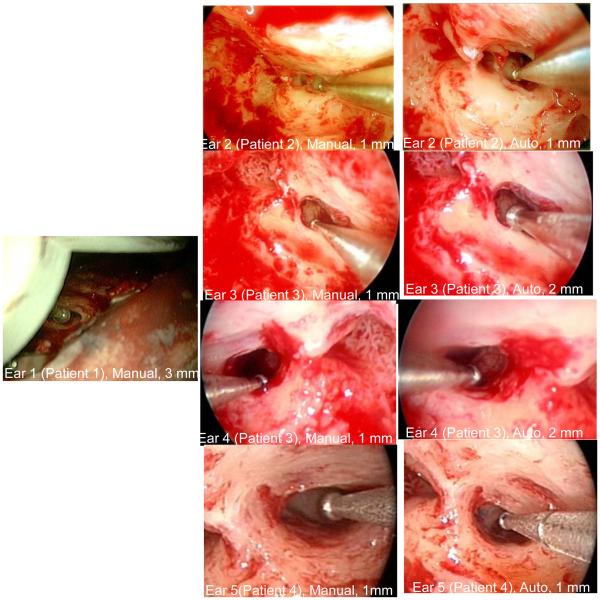
Results: All surgical paths successfully traversed the facial recess and hit the basal turn of the cochlea. Distance in millimeters (average +/- SD) from the midpoint of the drill to the facial nerve was 1.18 +/- 0.68 for the "manual" path and 1.24 +/- 0.44 mm for the "automatic" path and for the chorda tympani 0.986 +/- 0.48 for the "manual" path and 1.22 +/- 0.62 for the "automatic" path.
Conclusions: Percutaneous cochlear implant access using customized drill guides based on preoperative CT scans and image-guided surgery technology can be safely accomplished.
Figures

References
-
- Soper NJ, Barteau JA, Clayman RV, Ashley SW. Comparison of early postoperative results for laparoscopic versus standard open cholecystectomy. Surg Gynecol Obstet. 1992;174(2):114–118. - PubMed
-
- Vierra M. Minimally invasive surgery. Annu Rev Med. 1995;46:147–158. - PubMed
-
- Messerklinger W. Endoscopy of the nose. Urban&Schwarzenberg (Baltimore, Munich) 1978
-
- Draf W. Therapeutic endoscopy of the paranasal sinuses. Endoscopy. 1978;10(4):247–254. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
