

Early acute kidney injury and sepsis: a multicentre evaluation
- PMID: 18402655
- PMCID: PMC2447598
- DOI: 10.1186/cc6863
Early acute kidney injury and sepsis: a multicentre evaluation
Abstract
Introduction: We conducted a study to evaluate the incidence, risk factors and outcomes associated with early acute kidney injury (AKI) in sepsis.
Methods: The study was a retrospective interrogation of prospectively collected data from the Australian New Zealand Intensive Care Society Adult Patient Database. Data were collected from 57 intensive care units (ICUs) across Australia. In total, 120,123 patients admitted to ICU for more than 24 hours from 1 January 2000 to 31 December 2005 were included in the analysis. The main outcome measures were clinical and laboratory data and outcomes.
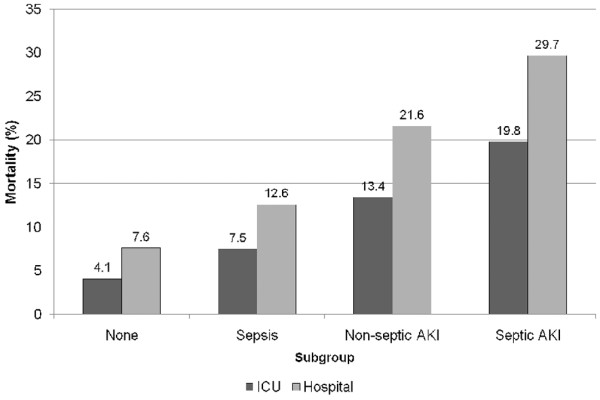
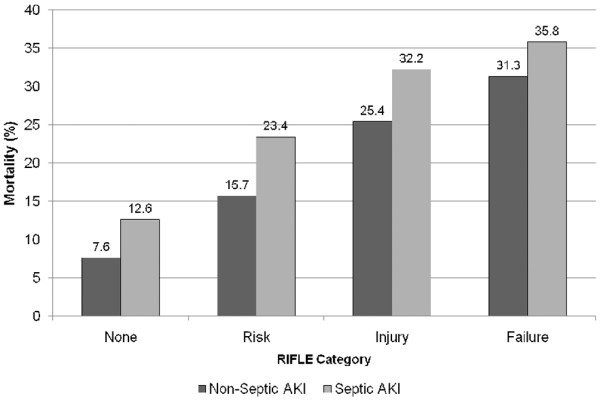
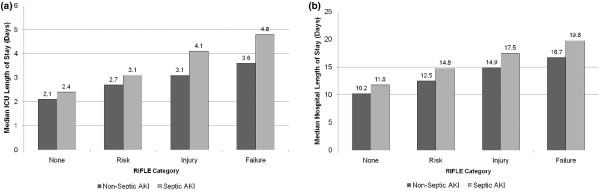
Results: Of 120,123 patients admitted, 33,375 had a sepsis-related diagnosis (27.8%). Among septic patients, 14,039 (42.1%) had concomitant AKI (septic AKI). Sepsis accounted for 32.4% of all patients with AKI. For septic AKI stratified by RIFLE (risk of renal failure, injury to the kidney, failure of kidney function, loss of kidney function and end-stage kidney disease) category, 38.5% of patients belonged to the risk category, 38.8% to the injury category and 22.7% to the failure category. Septic AKI patients had greater acuity of illness (P < 0.0001), lower blood pressure (P < 0.0001), higher heart rates (P < 0.0001), worse pulmonary function measures by arterial oxygen tension/fraction of inspired oxygen ratio (P < 0.0001), greater acidaemia (P < 0.0001) and higher white cell counts (P < 0.0001) compared with patients with nonseptic AKI. Septic AKI was also associated with greater severity of AKI (RIFLE category injury or failure) compared with nonseptic AKI. Septic AKI was associated with a significantly higher crude and co-variate adjusted mortality in the ICU (19.8% versus 13.4%; odds ratio 1.60, 95% confidence interval 1.5 to 1.7; P < 0.001) and in hospital (29.7% versus 21.6%; odds ratio 1.53, 95% confidence interval 1.46 to 1.60; P < 0.001) compared with nonseptic AKI. Septic AKI was associated with higher ICU and hospital mortality across all strata of RIFLE categories. Septic AKI patients had longer durations of stay in both ICU and hospital across all strata of RIFLE categories.
Conclusion: Septic AKI is common during the first 24 hours after ICU admission. Patients with septic AKI are generally sicker, with a higher burden of illness, and have greater abnormalities in acute physiology compared with patients with nonseptic AKI. Moreover, septic AKI is independently associated with higher odds of death and longer duration of hospitalization.
Figures
References
-
- Bagshaw SM, Laupland KB, Doig CJ, Mortis G, Fick GH, Mucenski M, Godinez-Luna T, Svenson LW, Rosenal T. Prognosis for long-term survival and renal recovery in critically ill patients with severe acute renal failure: a population-based study. Crit Care. 2005;9:R700–R709. doi: 10.1186/cc3879. - DOI - PMC - PubMed
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, Morgera S, Schetz M, Tan I, Bouman C, Macedo E, Gibney N, Tolwani A, Ronco C, Beginning and Ending Supportive Therapy for the Kidney (BEST Kidney) Investigators Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA. 2005;294:813–818. doi: 10.1001/jama.294.7.813. - DOI - PubMed
-
- Bagshaw SM, George C, Dinu I, Bellomo R. A multi-centre evaluation of the RIFLE criteria for early acute kidney injury in critically ill patients. Nephrol Dial Transplant. 2007 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
