

Laparoscopic management of symptomatic Meckel's diverticula: a simple tangential stapler excision
- PMID: 18402742
- PMCID: PMC3016022
Laparoscopic management of symptomatic Meckel's diverticula: a simple tangential stapler excision
Abstract
Background: Meckel's diverticulum was first described about 400 years ago and continues to be a rare congenital disorder. Laparoscopic surgery for Meckel's diverticulum has been described in mostly case reports. We present our series of patients with symptomatic Meckel's diverticulum.
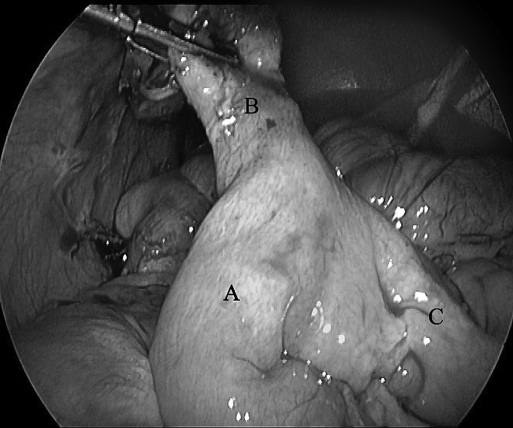
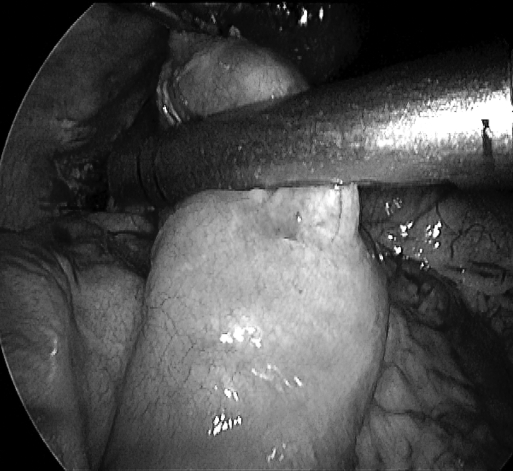
Methods: We have treated 12 patients with symptomatic Meckel's diverticulum from 1994 through 2006 at our institution. All the patients presented with features of either appendicitis or peritonitis, some with a vague abdominal mass. Clinical diagnosis of Meckel's diverticulum was made in only 4 patients. Diagnostic laparoscopy confirmed Meckel's diverticulitis in all patients. Laparoscopic stapler resection of the lesions was performed for all patients, tangential excision in 10 and wedge excision in 2.
Results: The incidence of Meckel's diverticulum at our institution is 0.3%. The majority of patients were male children. There were no staple-line leaks in any case. All patients recovered well postoperatively, and the day of discharge was in the range of the fourth to the seventh POD. Heterotopic gastric mucosa was found in the majority of the diverticula. Eight patients were followed up for 24 months, and 4 patients reported for follow-up after 45 months and were found to be symptom-free.
Discussion: The diagnosis of Meckel's diverticulitis is rarely made preoperatively. Surgical resection is indicated only if the diverticulum is symptomatic or if the base is narrow. Traditionally, open wedge resection (including the anterior wall of the ileum) of the diverticulum is the treatment. We think that a simple tangential stapler resection can also be performed, with good outcome.
Conclusion: Laparoscopy is useful in both diagnosis and treatment. Laparoscopic resection of Meckel's diverticulum is feasible and ideal, especially when performed in specialized centers.
Figures


References
-
- Shalaby RY, Soliman SM, Fawy M, Samaha A. Laparoscopic management of Meckel's diverticulum in children. J Pediatr Surg. 2005;40:562–567 - PubMed
-
- Schmid SW, Schafer M, Krahenbuhl L, Buchler MW. The role of laparoscopy in symptomatic Meckel's diverticulum. Surg Endosc. 1999;13:1047–1049 - PubMed
-
- Memon AA, Memon GA, Ansari AG, Ghumro AA. Symptomatic Meckel's diverticulum. JCPSP. 1999;9:476–479
-
- Ng WT, Wong MK, Kong CK, Chan YT. Laparoscopic approach to Meckel's diverticulectomy. Br J Surg. 1992;79:973–974 - PubMed
-
- Fansler RF. Laparoscopy in the management of Meckel's diverticulum. Surg Laparosc Endosc. 1996;6:231–233 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources