

Coronary atherosclerotic lesions in human immunodeficiency virus-infected patients: a histopathologic study
- PMID: 18402832
- PMCID: PMC7058188
- DOI: 10.1016/j.carpath.2007.12.011
Coronary atherosclerotic lesions in human immunodeficiency virus-infected patients: a histopathologic study
Abstract
Background: Studies suggest human immunodeficiency virus-positive (HIV+) patients have an increased risk of coronary artery disease (CAD), yet little is known about the histopathology, severity, or distribution of lesions.
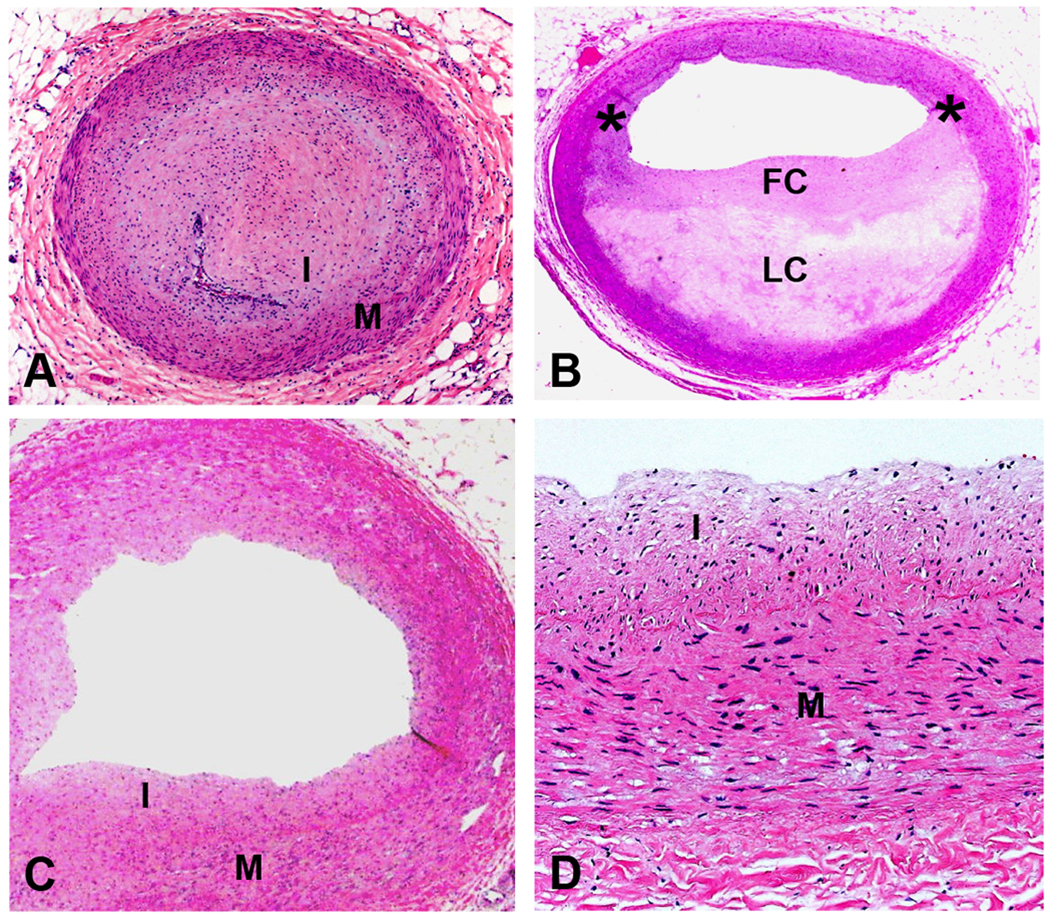
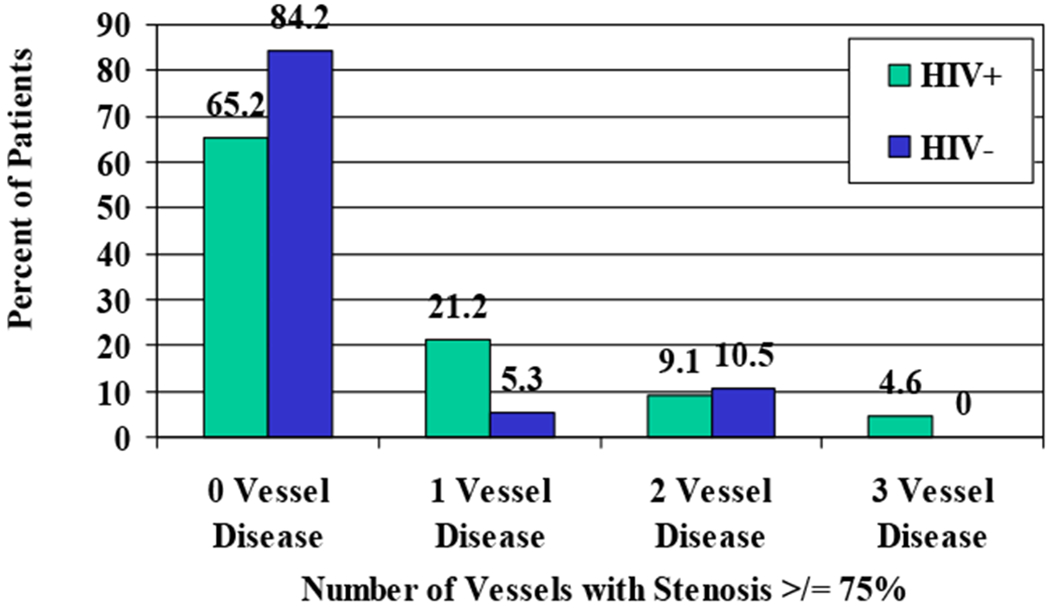
Methods: The coronary arteries of 66 deceased AIDS patients and 19 HIV controls (age <55) were dissected and graded for percent luminal stenosis by intimal lesions, percent of intima involved with lipid, and extent of intimal calcification on a scale of 0 to 3. Medical histories, antiretroviral therapies, and CAD risk factors were reviewed.
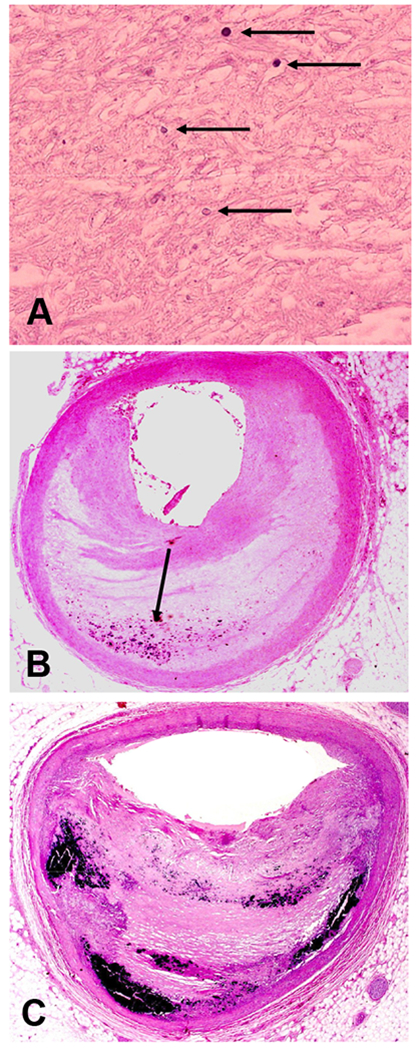
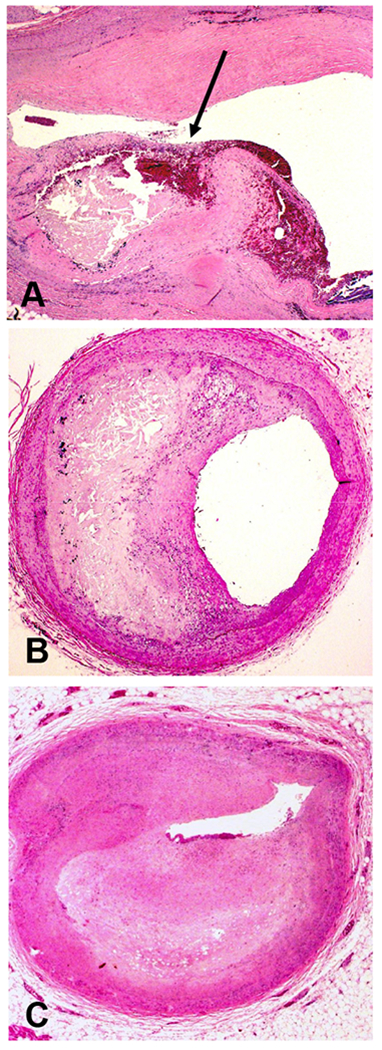
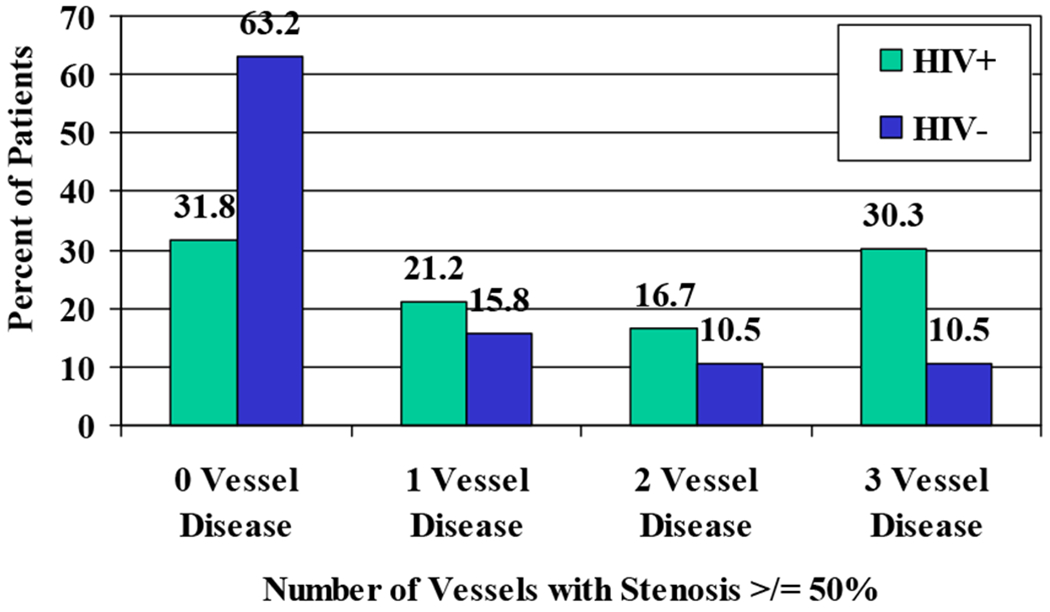
Results: HIV+ patients were older than controls (P=.06), and more were male (P=.02). Thirty-five percent of HIV+ patients had stenosis >or=75% of at least one artery. Compared to controls, HIV+ patients had three times greater odds of stenosis >or=75%, controlling for age and sex (one-sided P=.03). Older age and male sex were also risk factors (one-sided P<.001). HIV seropositivity was associated with increased plaque lipid content (one-sided P=.02) and calcification (one-sided P=.08). Duration of HIV infection, antiretroviral therapy, and immune status did not predict severe disease in multivariate analyses. Previously unreported patterns of dystrophic calcification were observed in HIV+ patients and older controls.
Conclusions: Young to middle-aged patients dying from advanced AIDS have atherosclerotic CAD that may result in luminal narrowing, heavy calcification, and high plaque lipid content. The pattern of disease, location of lesions, and plaque composition are typical of atherosclerosis in HIV-negative patients. No relationship between antiretroviral therapies and atherosclerosis was seen in this small study of heavily treated patients.
Figures
References
-
- Palella FJ Jr, Delaney KM, Moorman AC, Loveless MO, Fuhrer J, Satten GA, Aschman DJ, Holmberg SD. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med 1998; 338:853–60. - PubMed
-
- Friis-Moller N, Reiss P, Sabin CA, Weber R, Monforte A, El-Sadr W, Thiebaut R, De Wit S, Kirk O, Fontas E, Law MG, Phillips A, Lundgren JD. Class of antiretroviral drugs and the risk of myocardial infarction. N Engl J Med 2007; 356:1723–35. - PubMed
-
- Hsue PY, Lo JC, Franklin A, Bolger AF, Martin JN, Deeks SG, Waters DD. Progression of atherosclerosis as assessed by carotid intima-media thickness in patients with HIV infection. Circulation 2004; 109:1603–8. - PubMed
-
- Stein JH, Klein MA, Bellehumeur JL, McBride PE, Wiebe DA, Otvos JD, Sosman JM. Use of human immunodeficiency virus-1 protease inhibitors is associated with atherogenic lipoprotein changes and endothelial dysfunction. Circulation 2001; 104:257–62. - PubMed
-
- van Wijk JP, de Koning EJ, Cabezas MC, Joven J, op’t Roodt J, Rabelink TJ, Hoepelman AM. Functional and structural markers of atherosclerosis in human immunodeficiency virus-infected patients. J Am Coll Cardiol 2006; 47:1117–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
