

Computer-delivered interventions for health promotion and behavioral risk reduction: a meta-analysis of 75 randomized controlled trials, 1988-2007
- PMID: 18403003
- PMCID: PMC2572996
- DOI: 10.1016/j.ypmed.2008.02.014
Computer-delivered interventions for health promotion and behavioral risk reduction: a meta-analysis of 75 randomized controlled trials, 1988-2007
Abstract
Objective: The use of computers to promote healthy behavior is increasing. To evaluate the efficacy of these computer-delivered interventions, we conducted a meta-analysis of the published literature.
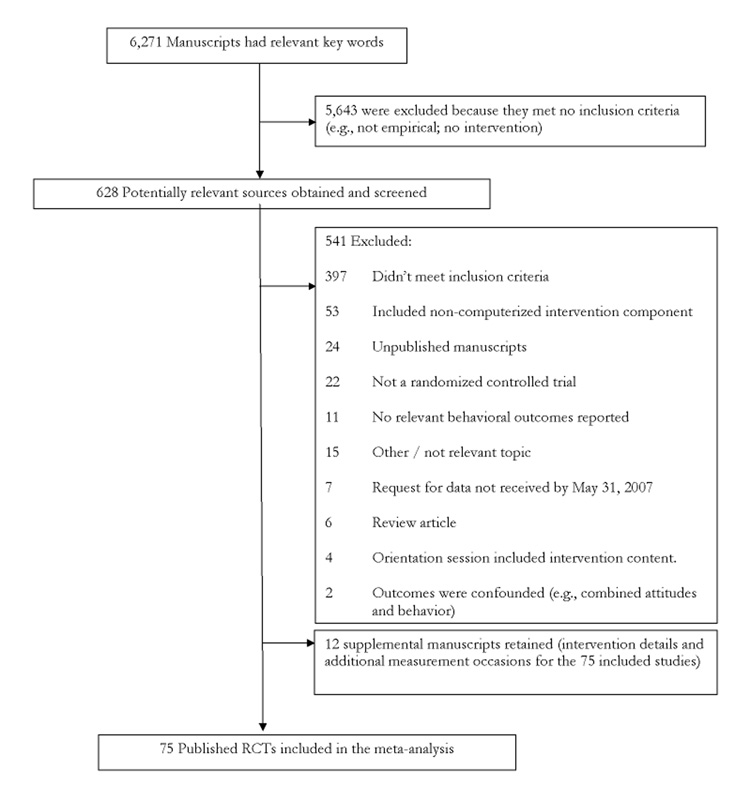
Method: Studies examining health domains related to the leading health indicators outlined in Healthy People 2010 were selected. Data from 75 randomized controlled trials, published between 1988 and 2007, with 35,685 participants and 82 separate interventions were included. All studies were coded independently by two raters for study and participant characteristics, design and methodology, and intervention content. We calculated weighted mean effect sizes for theoretically-meaningful psychosocial and behavioral outcomes; moderator analyses determined the relation between study characteristics and the magnitude of effect sizes for heterogeneous outcomes.
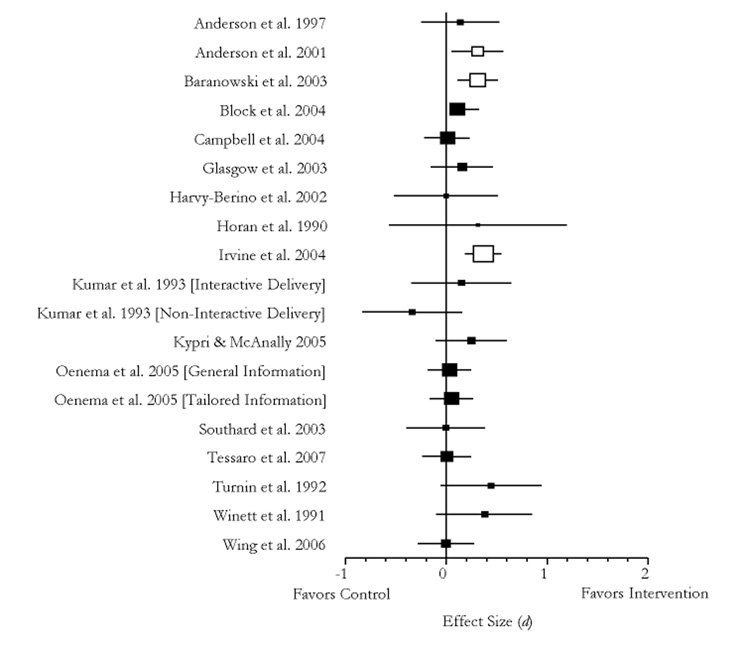
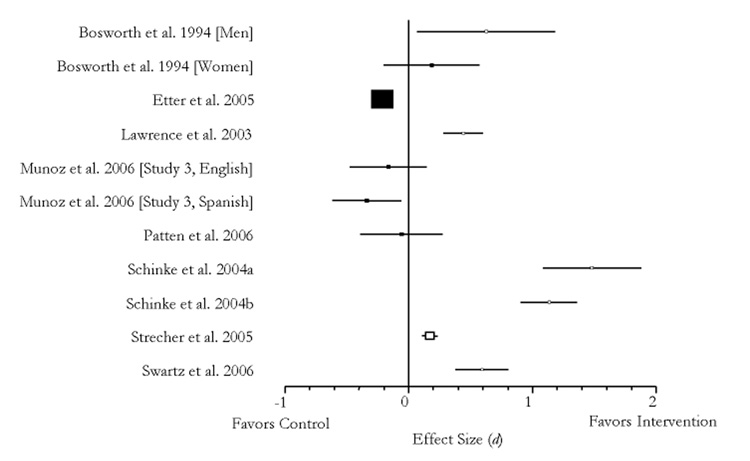
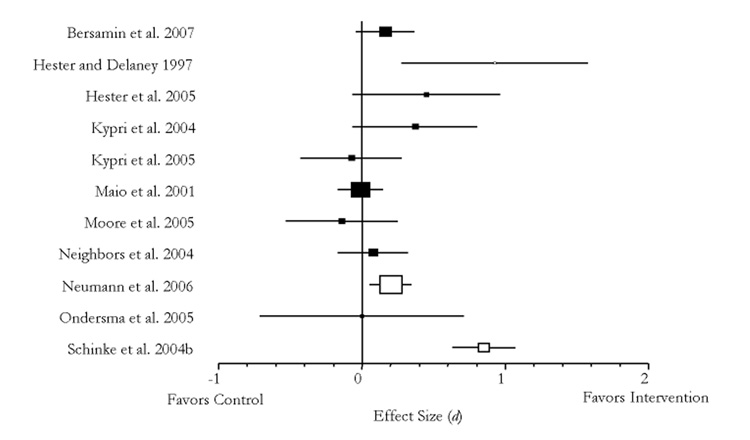
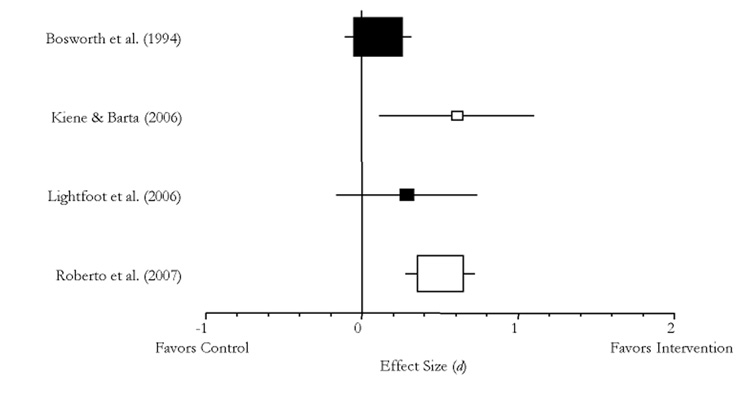
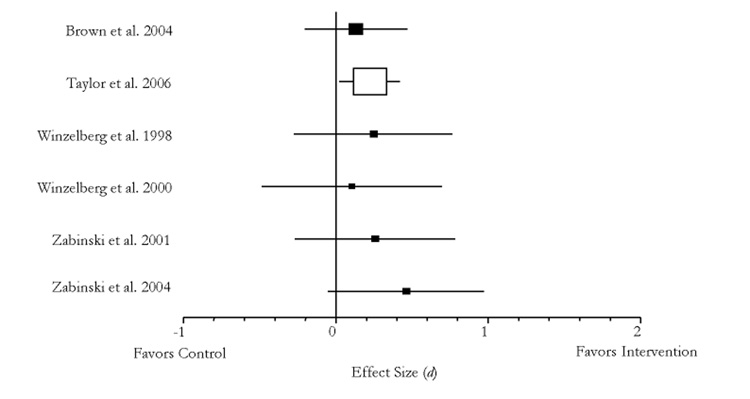
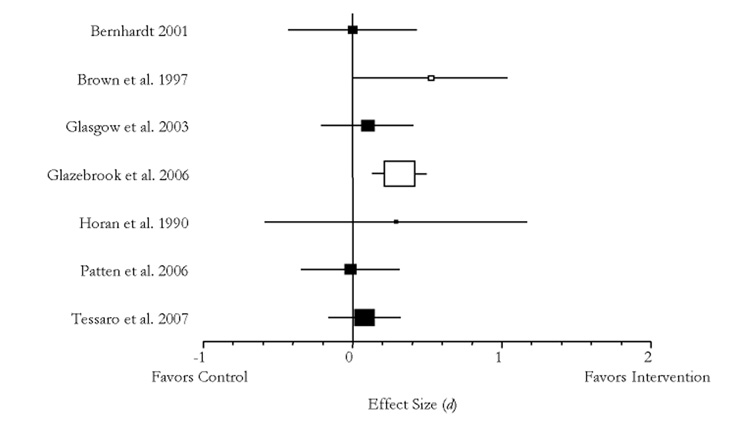
Results: Compared with controls, participants who received a computer-delivered intervention improved several hypothesized antecedents of health behavior (knowledge, attitudes, intentions); intervention recipients also improved health behaviors (nutrition, tobacco use, substance use, safer sexual behavior, binge/purge behaviors) and general health maintenance. Several sample, study and intervention characteristics moderated the psychosocial and behavioral outcomes.
Conclusion: Computer-delivered interventions can lead to improved behavioral health outcomes at first post-intervention assessment. Interventions evaluating outcomes at extended assessment periods are needed to evaluate the longer-term efficacy of computer-delivered interventions.
Figures
References
-
- Alterman AI, Baughman TG. Videotape versus computer interactive education in alcoholic and nonalcoholic controls. Alcohol Clin Exp Res. 1991;15:39–44. - PubMed
-
- American Lung Association. Trends in tobacco use. 2007. [Online]. Available from: http://www.lungusa.org/site/pp.asp?c=dvLUK9O0E&b=33347 [cited 12 September 2007]
-
- Anderson ES, Winett RA, Bickley PG, Walberg-Rankin J, Moore JF, Leahy M, Harris CE, Gerkin RE. The effects of a multimedia system in supermarkets to alter shoppers' food purchases. J Health Psych. 1997;2:209–223. - PubMed
-
- Anderson ES, Winett RA, Wojcik JR, Winett SG, Bowden T. A computerized social cognitive intervention for nutrition behavior: direct and mediated effects on fat, fiber, fruits, and vegetables, self-efficacy, and outcome expectations among food shoppers. Ann Behav Med. 2001;23:88–100. - PubMed
-
- Andrewes DG, O'Connor P, Mulder C, McLennan J, Derham H, Weigall S, Say S. Computerised psychoeducation for patients with eating disorders. Aust NZ J Psychiat. 1996;30:492–497. - PubMed
Supplemental References for the Studies Included in the Meta-Analysis
-
- Brown JLB. PhD thesis. Stanford University; 2002. An evaluation of an internet-delivered eating disorder prevention program for adolescents and their parents. [Additional study information for Brown et al. 2004] - PubMed
-
- Feil EG, Glasgow RE, Boles S, McKay HG. Who participates in internet-based self-management programs? A study among novice computer users in a primary care setting. Diabetes Educator. 2000;26:806–811. [Additional study information for Glasgow et al. 2003] - PubMed
-
- Hawkins RP, Gustafson DH, Chewning B, Bosworth K, Day PM. Reaching hard-to-reach populations. Interactive computer programs as public information campaigns for adolescents. J Commun. 1987;37:8–28. [Additional study information for Bosworth et al. 1994]
-
- Kosma M. PhD thesis. Oregon State University; 2003. Interactive vs. non-interactive electronically delivered motivational materials for physical activity initiation and enhancement among adults with physical disabilities. [Additional study information for Kosma et al. 2005]
-
- Lawrence T, Aveyard P, Cheng KK, Griffin C, Johnson C, Croghan E. Does stage-based smoking cessation advice in pregnancy result in long-term quitters? An 18-month postpartum follow-up of a randomized controller trial. Addiction. 2005;100:107–116. [Additional measurement occasion for Lawrence et al 2003] - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
