

Gastric endoscopy in the 21st century: appropriate use of an invasive procedure in the era of non-invasive testing
- PMID: 18403275
- PMCID: PMC2525514
- DOI: 10.1016/j.dld.2008.02.032
Gastric endoscopy in the 21st century: appropriate use of an invasive procedure in the era of non-invasive testing
Abstract
Background: The acceptance of the premise that Helicobacter pylori infection is aetiologically related to gastric cancer and peptic ulcer and that the risk of gastric cancer among Helicobacter pylori infected individuals is related to the extent, severity and duration of atrophic gastritis has led to major changes in medical and endoscopic practices. The development of non-invasive methods to detect Helicobacter pylori and to estimate the extent and severity of gastritis has reduced the need for diagnostic endoscopy in asymptomatic individuals.
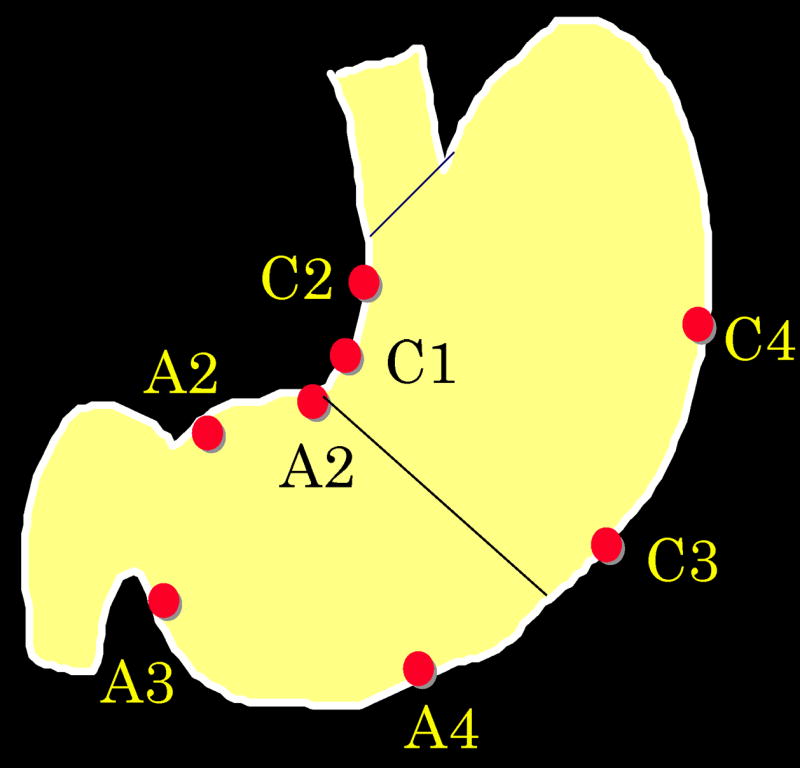
Methods and results: Here we provide recommendations regarding deciding whether non-invasive and endoscopic assessment of the gastric mucosa is preferred. We also include specific recommendations and caveats regarding the preferred biopsy number and sites as well as the identification of specimens, to allow the pathologist to reliable stage the severity and extent of gastritis, and thus provide prognostic information needed for patient managements (e.g., whether endoscopic surveillance is recommended).
Conclusion: In summary, while there is clearly a role for gastric endoscopy and endoscopic biopsy in the Helicobacter pylori era, obtaining useful diagnostic and prognostic information is critically dependent upon attention to detail with regard to biopsy site and identification as to the location from where the specimen was taken.
Conflict of interest statement
Conflict of interest statements
Dr. Graham has received small amounts of grant support and/or free drugs or urea breath tests from Meretek, Jannsen/Eisai, and TAP, and BioHit for investigator initiated and completely investigator controlled research. Dr. Graham is a consultant for Novartis in relation to vaccine development for treatment or prevention of
Figures


Similar articles
-
Helicobacter pylori (Hp) IgG ELISA of the New-Generation GastroPanel® Is Highly Accurate in Diagnosis of Hp-Infection in Gastroscopy Referral Patients.Anticancer Res. 2020 Nov;40(11):6387-6398. doi: 10.21873/anticanres.14660. Anticancer Res. 2020. PMID: 33109577 Clinical Trial.
-
AGA Clinical Practice Update on Screening and Surveillance in Individuals at Increased Risk for Gastric Cancer in the United States: Expert Review.Gastroenterology. 2025 Feb;168(2):405-416.e1. doi: 10.1053/j.gastro.2024.11.001. Epub 2024 Dec 23. Gastroenterology. 2025. PMID: 39718517 Review.
-
Operative link on gastritis assessment stage is an appropriate predictor of early gastric cancer.World J Gastroenterol. 2016 Apr 7;22(13):3670-8. doi: 10.3748/wjg.v22.i13.3670. World J Gastroenterol. 2016. PMID: 27053859 Free PMC article.
-
Helicobacter pylori Infection, Gastric Cancer and Gastropanel.Rom J Intern Med. 2016 Sep 1;54(3):151-156. doi: 10.1515/rjim-2016-0025. Rom J Intern Med. 2016. PMID: 27658162 Review.
-
[ANALYSIS OF THE RESULTS OF ENDOSCOPIC AND MORPHOLOGICAL STUDIES OF THE STOMACH MUCOSA WITH REDUCED PEPSINOGEN-I IN PATIENTS WITH H. PYLORI (H.P.)--ASSOCIATED GASTRITIS IN TOMSK AND TOMSK REGION].Eksp Klin Gastroenterol. 2015;(4):66-70. Eksp Klin Gastroenterol. 2015. PMID: 26415268 Russian.
Cited by
-
Operative link for gastritis assessment vs operative link on intestinal metaplasia assessment.World J Gastroenterol. 2011 Nov 7;17(41):4596-601. doi: 10.3748/wjg.v17.i41.4596. World J Gastroenterol. 2011. PMID: 22147965 Free PMC article.
-
Histomorphological Characteristics and Pathological Types of Hyperproliferation of Gastric Surface Epithelial Cells.Gastroenterol Res Pract. 2021 Mar 9;2021:8828326. doi: 10.1155/2021/8828326. eCollection 2021. Gastroenterol Res Pract. 2021. PMID: 33777138 Free PMC article.
-
Pyloric metaplasia, pseudopyloric metaplasia, ulcer-associated cell lineage and spasmolytic polypeptide-expressing metaplasia: reparative lineages in the gastrointestinal mucosa.J Pathol. 2018 Jun;245(2):132-137. doi: 10.1002/path.5066. Epub 2018 Apr 14. J Pathol. 2018. PMID: 29508389 Free PMC article.
-
Guilt by association: intestinal metaplasia does not progress to gastric cancer.Curr Opin Gastroenterol. 2018 Nov;34(6):458-464. doi: 10.1097/MOG.0000000000000472. Curr Opin Gastroenterol. 2018. PMID: 30138135 Free PMC article. Review.
-
Panel of serum biomarkers (GastroPanel) in diagnosis of atrophic gastritis and Helicobacter pylori infection: a protocol of systematic review and meta-analysis.BMJ Open. 2022 Sep 28;12(9):e062849. doi: 10.1136/bmjopen-2022-062849. BMJ Open. 2022. PMID: 36171026 Free PMC article.
References
-
- Wilber DL. The history of diseases of the stomach and duodenum with reference also to their etiology. In: Eusterman GB, Balfour DC, editors. The stomach and duodenum. Philadelphia: W.B. Saunders Company; 1935. pp. 1–21.
-
- Graham DY, Uemura N. Natural history of gastric cancer after Helicobacter pylori eradication in Japan: after endoscopic resection, after treatment of the general population, and naturally. Helicobacter. 2006;11:139–143. - PubMed
-
- Sipponen P, Graham DY. Importance of atrophic gastritis in diagnostics and prevention of gastric cancer: application of plasma biomarkers. Scand J Gastroenterol. 2007;42:2–10. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
