

Review
doi: 10.1136/bmj.39513.555150.BE.
Catheter ablation for atrial fibrillation
Affiliations
- PMID: 18403546
- PMCID: PMC2292272
- DOI: 10.1136/bmj.39513.555150.BE
Item in Clipboard
Review
Catheter ablation for atrial fibrillation
BMJ.
.
No abstract available
Conflict of interest statement
Competing interests: AF consults for and has received honorariums from Medtronic and receives research support from St Jude Medical.
Figures
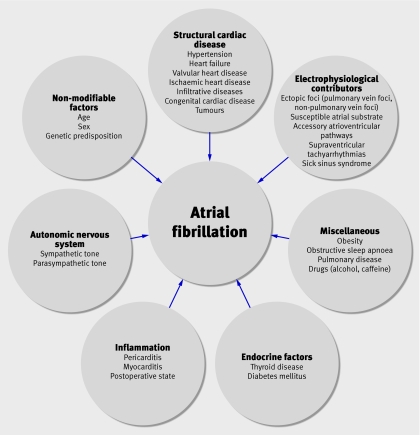
Fig 1 Factors contributing to development of atrial fibrillation. Clinical factors predisposing patients to atrial fibrillation are complex and may be inter-related. *These conditions may result in structural changes such as left atrial enlargement or stretch, myocardial hypertrophy, or left ventricular systolic dysfunction
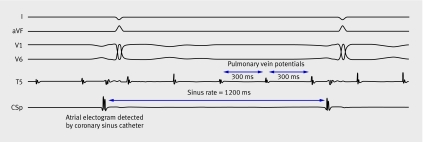
Fig 2 Intracardiac electrogram (recorded at a paper speed of 100 mm/s) from a patient with paroxysmal atrial fibrillation undergoing pulmonary vein isolation. Patient is in sinus rhythm at 50 bpm (cycle length=1200 ms), seen on surface electrograms (I, aVF, V1, V6). An intracardiac atrial electrogram is detected at the same cycle length by a catheter in the coronary sinus, preceding the surface electrogram deflection. A circular lasso catheter in the left upper pulmonary vein (T5) records pulmonary vein potentials occurring at a cycle length of 300 ms and dissociated from sinus activity. Other measurement points from lasso catheter were removed for simplicity
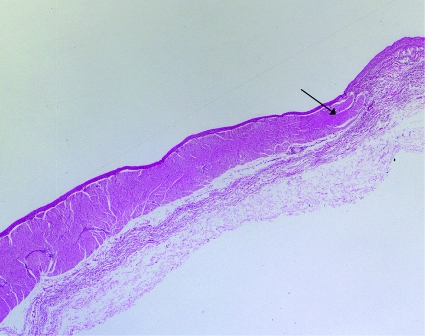
Fig 3 Muscular sleeves extending into pulmonary vein. Specimen from pulmonary vein showing muscular sleeves (arrowhead) extending from left atrium into pulmonary vein. Haematoxylin and eosin, ×2 magnification

Fig 4 Electroanatomical map of left atrium in patient with persistent atrial fibrillation undergoing pulmonary vein isolation. Computed tomogram before ablation procedure is merged with three dimensional electroanatomical map of left atrium created during ablation. Left atrium is viewed from a posterior (panel A) and superior (panel B) orientation, with left atrium appendage on left. Dots represent sites of delivery of radiofrequency energy. Radiofrequency lesions encircle both left and right pulmonary veins, avoiding posterior wall of left atrium, and a line of radiofrequency ablation is seen along the mitral isthmus (region extending from left inferior pulmonary vein to mitral annulus)
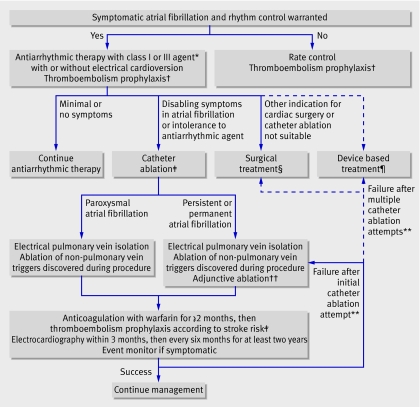
Fig 5 Proposed algorithm for management of symptomatic patients with atrial fibrillation referred for rhythm control. Solid lines represent established pathways supported by clinical evidence, guidelines, or expert consensus documents. Dashed lines represent less established pathways. *Appropriate antiarrhythmic drug therapy is outlined in practice guidelines. †Underlying stroke risk can be assessed using the CHADS2 score; one point each is assigned for a history of heart failure, hypertension, age >75, diabetes mellitus, and two points for previous cerebral ischaemia. Aspirin is generally recommended if the score is 0, aspirin or warfarin if the score is 1, and warfarin if the score is ≥2. ‡First line therapy with catheter ablation may be appropriate for patients in whom long term antiarrhythmic drug therapy may be harmful or for those who want to avoid antiarrhythmic drugs. Presence of a left atrial thrombus is an absolute contraindication to catheter ablation. §Summary of surgical techniques for restoration of atrial fibrillation can be found in Heart Rhythm Society consensus document. ¶Potential measures include permanent pacing or implantable atrial defibrillators for restoration of sinus rhythm. **Repeat catheter ablations should generally be delayed until at least three months after the initial procedure. No consensus exists on what constitutes the maximum number for repeat attempts. ††Substrate ablation in form of linear ablation, or ablation of complex fractionated electrograms or sites of autonomic innervation. Adjunctive ablation may be appropriate in patients with paroxysmal atrial fibrillation in whom an initial attempt has been unsuccessful
References
-
- Fuster V, Ryden LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation 2006;114:e257-354. - PubMed
-
- Cappato R, Calkins H, Chen SA, Davies W, Iesaka Y, Kalman J, et al. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation 2005;111:1100-5. - PubMed
-
- Nathan H, Eliakim M. The junction between the left atrium and the pulmonary veins. An anatomic study of human hearts. Circulation 1966;34:412-22. - PubMed
-
- Haissaguerre M, Jais P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med 1998;339:659-66. - PubMed
-
- Haissaguerre M, Shah DC, Jais P, Hocini M, Yamane T, Deisenhofer I, et al. Electrophysiological breakthroughs from the left atrium to the pulmonary veins. Circulation 2000;102:2463-5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical