

Shared genetic causes of cardiac hypertrophy in children and adults
- PMID: 18403758
- PMCID: PMC2752150
- DOI: 10.1056/NEJMoa075463
Shared genetic causes of cardiac hypertrophy in children and adults
Abstract
Background: The childhood onset of idiopathic cardiac hypertrophy that occurs without a family history of cardiomyopathy can portend a poor prognosis. Despite morphologic similarities to genetic cardiomyopathies of adulthood, the contribution of genetics to childhood-onset hypertrophy is unknown.
Methods: We assessed the family and medical histories of 84 children (63 boys and 21 girls) with idiopathic cardiac hypertrophy diagnosed before 15 years of age (mean [+/-SD] age, 6.99+/-6.12 years). We sequenced eight genes: MYH7, MYBPC3, TNNT2, TNNI3, TPM1, MYL3, MYL2, and ACTC. These genes encode sarcomere proteins that, when mutated, cause adult-onset cardiomyopathies. We also sequenced PRKAG2 and LAMP2, which encode metabolic proteins; mutations in these genes can cause early-onset ventricular hypertrophy.
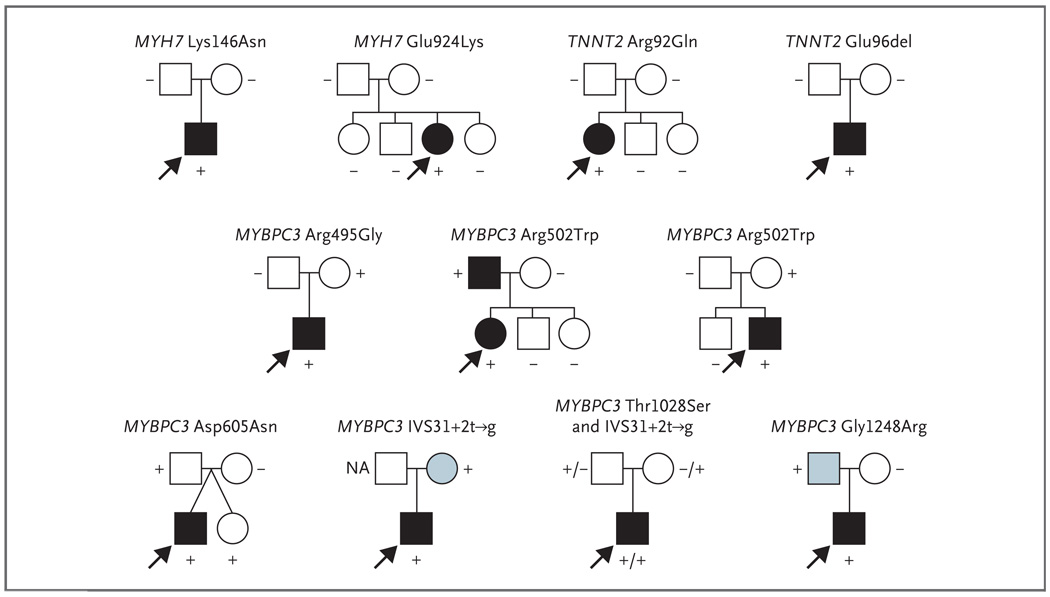
Results: We identified mutations in 25 of 51 affected children without family histories of cardiomyopathy and in 21 of 33 affected children with familial cardiomyopathy. Among 11 of the 25 children with presumed sporadic disease, 4 carried new mutations and 7 inherited the mutations. Mutations occurred predominantly (in >75% of the children) in MYH7 and MYBPC3; significantly more MYBPC3 missense mutations were detected than occur in adult-onset cardiomyopathy (P<0.005). Neither hypertrophic severity nor contractile function correlated with familial or genetic status. Cardiac transplantation and sudden death were more prevalent among mutation-positive than among mutation-negative children; implantable cardioverter-defibrillators were more frequent (P=0.007) in children with family histories that were positive for the mutation.
Conclusions: Genetic causes account for about half of presumed sporadic cases and nearly two thirds of familial cases of childhood-onset hypertrophy. Childhood-onset hypertrophy should prompt genetic analyses and family evaluations.
Copyright 2008 Massachusetts Medical Society.
Figures
References
-
- Lipshultz SE, Sleeper LA, Towbin JA, et al. The incidence of pediatric cardiomyopathy in two regions of the United States. N Engl J Med. 2003;348:1647–1655. - PubMed
-
- Nugent AW, Daubeney PE, Chondros P, et al. The epidemiology of childhood cardiomyopathy in Australia. N Engl J Med. 2003;348:1639–1646. - PubMed
-
- Nugent AW, Daubeney PE, Chondros P, et al. Clinical features and outcomes of childhood hypertrophic cardiomyopathy: results from a national population-based study. Circulation. 2005;112:1332–1338. - PubMed
-
- Colan SD, Lipshultz SE, Lowe AM, et al. Epidemiology and cause-specific outcome of hypertrophic cardiomyopathy in children: findings from the Pediatric Cardiomyopathy Registry. Circulation. 2007;115:773–781. - PubMed
-
- Yetman AT, McCrindle BW. Management of pediatric hypertrophic cardiomyopathy. Curr Opin Cardiol. 2005;20:80–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous