

Differential effects of biologic versus bisphosphonate inhibition of wear debris-induced osteolysis assessed by longitudinal micro-CT
- PMID: 18404739
- PMCID: PMC2742224
- DOI: 10.1002/jor.20620
Differential effects of biologic versus bisphosphonate inhibition of wear debris-induced osteolysis assessed by longitudinal micro-CT
Abstract
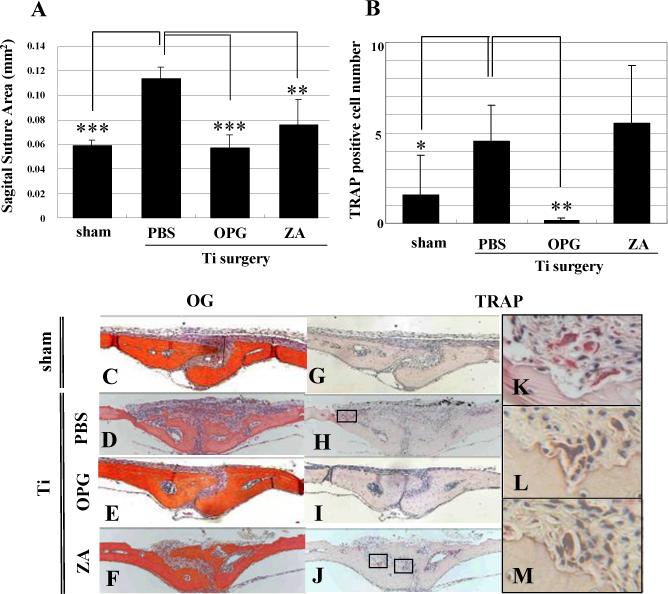
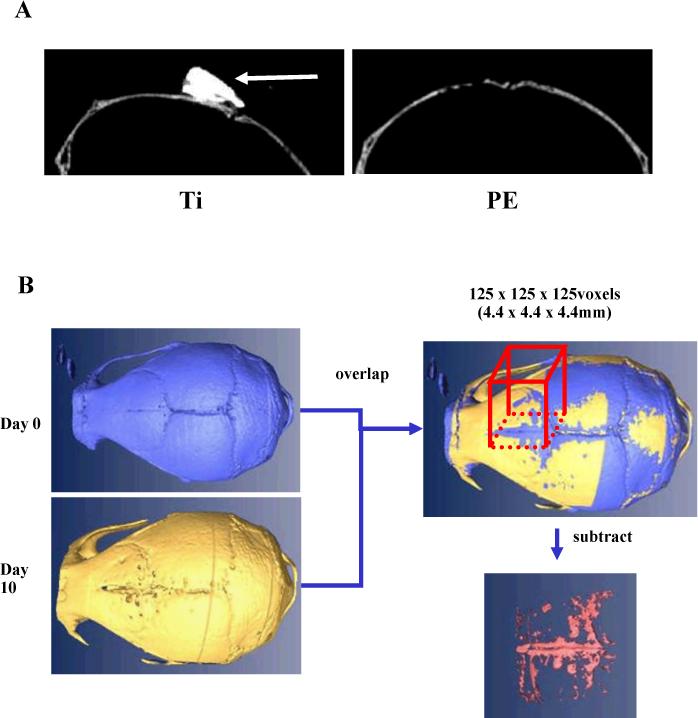
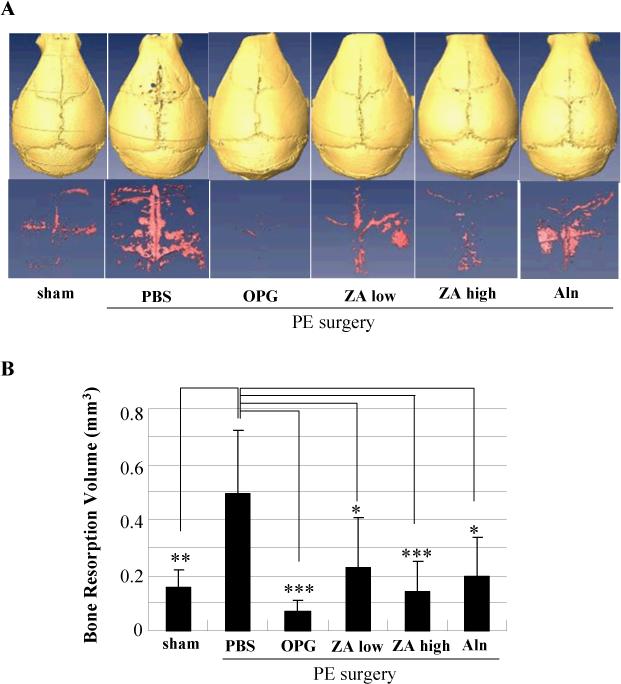
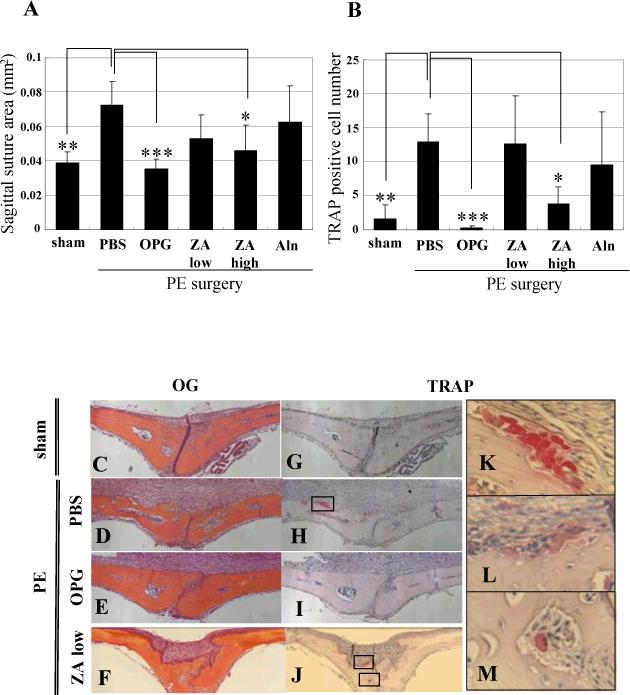
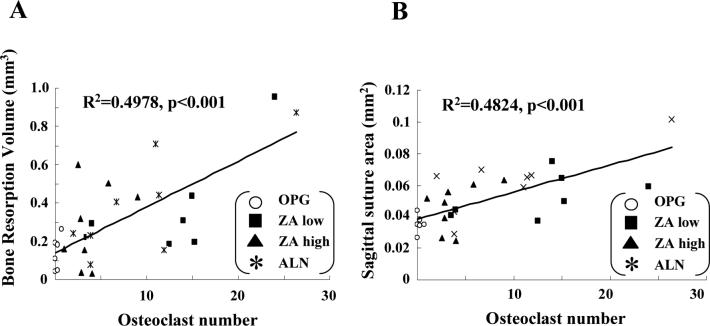
Aseptic loosening of total joint replacements is caused by wear debris-induced osteoclastic bone resorption, for which bisphosphonates (BPs) and RANK antagonists have been developed. Although BPs are effective in preventing metabolic bone loss, they are less effective for inflammatory bone loss. Because this difference has been attributed to the antiapoptotic inflammatory signals that protect osteoclasts from BP-induced apoptosis, but not RANK antagonists, we tested the hypothesis that osteoprotegerin (OPG) is more effective in preventing wear debris-induced osteolysis than zoledronic acid (ZA) or alendronate (Aln) in the murine calvaria model using in vivo micro-CT and traditional histology. Although micro-CT proved to be incompatible with titanium (Ti) particles, we were able to demonstrate a 3.2-fold increase in osteolytic volume over 10 days induced by polyethylene (PE) particles versus sham controls (0.49 +/- 0.23 mm(3) versus 0.15 +/- 0.067 mm(3); p < 0.01). Although OPG and high-dose ZA completely inhibited this PE-induced osteolysis (p < 0.001), pharmacological doses of ZA and Aln were less effective but still reached statistical significance (p < 0.05). Traditional histomorphometry of the sagital suture area of calvaria from both Ti and PE-treated mice confirmed the remarkable suppression of resorption by OPG (p < 0.001) versus the lack of effect by physiological BPs. The differences in drug effects on osteolysis were largely explained by the significant difference in osteoclast numbers observed between OPG versus BPs in both Ti- and PE-treated calvaria; and linear regression analyses that demonstrated a highly significant correlation between osteolysis volume and sagittal suture area versus osteoclast numbers (p < 0.001).
(c) 2008 Orthopaedic Research Society.
Figures
Similar articles
-
Efficacy of ex vivo OPG gene therapy in preventing wear debris induced osteolysis.J Orthop Res. 2002 Mar;20(2):169-73. doi: 10.1016/S0736-0266(01)00083-3. J Orthop Res. 2002. PMID: 11918293
-
Recombinant adeno-associated virus-mediated osteoprotegerin gene therapy inhibits wear debris-induced osteolysis.J Bone Joint Surg Am. 2002 Aug;84(8):1405-12. doi: 10.2106/00004623-200208000-00016. J Bone Joint Surg Am. 2002. PMID: 12177271
-
Quantitative small-animal surrogate to evaluate drug efficacy in preventing wear debris-induced osteolysis.J Orthop Res. 2000 Nov;18(6):849-55. doi: 10.1002/jor.1100180602. J Orthop Res. 2000. PMID: 11192243
-
Theaflavin-3,3'-digallate represses osteoclastogenesis and prevents wear debris-induced osteolysis via suppression of ERK pathway.Acta Biomater. 2017 Jan 15;48:479-488. doi: 10.1016/j.actbio.2016.11.022. Epub 2016 Nov 9. Acta Biomater. 2017. PMID: 27838465
-
Anti-oxidation treatment of ultra high molecular weight polyethylene components to decrease periprosthetic osteolysis: evaluation of osteolytic and osteogenic properties of wear debris particles in a murine calvaria model.Curr Rheumatol Rep. 2013 May;15(5):325. doi: 10.1007/s11926-013-0325-3. Curr Rheumatol Rep. 2013. PMID: 23532463 Free PMC article. Review.
Cited by
-
Inhibiting wear particles-induced osteolysis with naringin.Int Orthop. 2013 Jan;37(1):137-43. doi: 10.1007/s00264-012-1668-5. Epub 2012 Oct 31. Int Orthop. 2013. PMID: 23111634 Free PMC article.
-
PGE2 signaling through the EP4 receptor on fibroblasts upregulates RANKL and stimulates osteolysis.J Bone Miner Res. 2009 Oct;24(10):1753-62. doi: 10.1359/jbmr.090412. J Bone Miner Res. 2009. PMID: 19419302 Free PMC article.
-
Combination gene therapy targeting on interleukin-1β and RANKL for wear debris-induced aseptic loosening.Gene Ther. 2013 Feb;20(2):128-35. doi: 10.1038/gt.2012.1. Epub 2012 Feb 9. Gene Ther. 2013. PMID: 22318091 Free PMC article.
-
rna interference targeting p110β reduces tumor necrosis factor-alpha production in cellular response to wear particles in vitro and osteolysis in vivo.Inflammation. 2013 Oct;36(5):1041-54. doi: 10.1007/s10753-013-9636-9. Inflammation. 2013. PMID: 23584990
-
Titanium Wear Particles Exacerbate S. epidermidis-Induced Implant-Related Osteolysis and Decrease Efficacy of Antibiotic Therapy.Microorganisms. 2021 Sep 13;9(9):1945. doi: 10.3390/microorganisms9091945. Microorganisms. 2021. PMID: 34576840 Free PMC article.
References
-
- Purdue PE, Koulouvaris P, Potter HG, Nestor BJ, Sculco TP. The cellular and molecular biology of periprosthetic osteolysis. Clin Orthop Relat Res. 2007;454:251–61. - PubMed
-
- Agarwal S. Osteolysis: basic science, incidence and diagnosis. Curr Orthop. 2004;18:220–31.
-
- Rodan GA, Martin TJ. Therapeutic approaches to bone diseases. Science. 2000;289−5484:1508–14. - PubMed
-
- Boyle WJ, Simonet WS, Lacey DL. Osteoclast differentiation and activation. Nature. 2003;423−6937:337–42. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
