

Comparison of CT and MRI for presurgical characterization of paraaortic lymph nodes in patients with pancreatico-biliary carcinoma
- PMID: 18407595
- PMCID: PMC2703846
- DOI: 10.3748/wjg.14.2208
Comparison of CT and MRI for presurgical characterization of paraaortic lymph nodes in patients with pancreatico-biliary carcinoma
Abstract
Aim: To determine the accuracy of computed tomography (CT) and magnetic resonance (MR) for presurgical characterization of paraaortic lymph nodes in patients with pancreatico-biliary carcinoma.
Methods: Two radiologists independently evaluated CT and MR imaging of 31 patients who had undergone lymphadenectomy (9 metastatic and 22 non-metastatic paraaortic nodes). Receiver operating characteristic (ROC) curve analysis was performed using a five point scale to compare CT with MRI. To re-define the morphologic features of metastatic nodes, we evaluated CT scans from 70 patients with 23 metastatic paraaortic nodes and 47 non-metastatic ones. The short axis diameter, ratio of the short to long axis, shape, and presence of necrosis were compared between metastatic and non-metastatic nodes by independent samples t-test and Fisher's exact test. P < 0.05 was considered statistically significant.
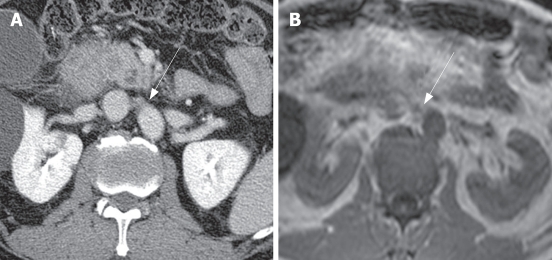
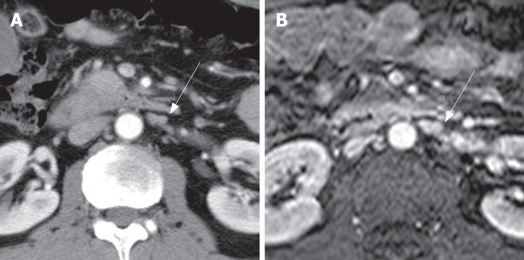
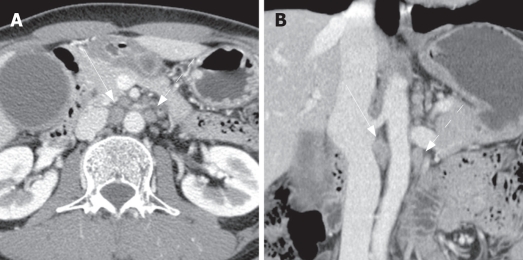
Results: The mean area under the ROC curve for CT (0.732 and 0.646, respectively) was slightly higher than that for MRI (0.725 and 0.598, respectively) without statistical significance (P = 0.940 and 0.716, respectively). The short axis diameter of the metastatic lymph nodes (mean = 9.2 mm) was significantly larger than that of non-metastatic ones (mean = 5.17 mm, P < 0.05). Metastatic nodes had more irregular margins (44.4%) and central necrosis (22.2%) than non-metastatic ones (9% and 0%, respectively), with statistical significance (P < 0.05).
Conclusion: The accuracy of CT scan for the characterization of paraaortic nodes is not different from that of MRI. A short axis-diameter (> 5.3 mm), irregular margin, and presence of central necrosis are the suggestive morphologic features of metastatic paraaortic nodes.
Figures
References
-
- Yoshida T, Matsumoto T, Sasaki A, Shibata K, Aramaki M, Kitano S. Outcome of paraaortic node-positive pancreatic head and bile duct adenocarcinoma. Am J Surg. 2004;187:736–740. - PubMed
-
- Shimada K, Sakamoto Y, Sano T, Kosuge T. The role of paraaortic lymph node involvement on early recurrence and survival after macroscopic curative resection with extended lymphadenectomy for pancreatic carcinoma. J Am Coll Surg. 2006;203:345–352. - PubMed
-
- Niedergethmann M, Rexin M, Hildenbrand R, Knob S, Sturm JW, Richter A, Post S. Prognostic implications of routine, immunohistochemical, and molecular staging in resectable pancreatic adenocarcinoma. Am J Surg Pathol. 2002;26:1578–1587. - PubMed
-
- Miyazaki K. Surgical strategy based on the spread mode of gallbladder carcinoma. Nippon Geka Gakkai Zasshi. 2005;106:286–290. - PubMed
-
- Kondo S, Nimura Y, Hayakawa N, Kamiya J, Nagino M, Kanai M, Uesaka K, Yuasa N, Sano T. Value of paraaortic lymphadenectomy for gallbladder carcinoma. Nippon Geka Gakkai Zasshi. 1998;99:728–732. - PubMed
