

The effects of involving a nurse practitioner in primary care for adult patients with urinary incontinence: the PromoCon study (Promoting Continence)
- PMID: 18412964
- PMCID: PMC2386786
- DOI: 10.1186/1472-6963-8-84
The effects of involving a nurse practitioner in primary care for adult patients with urinary incontinence: the PromoCon study (Promoting Continence)
Abstract
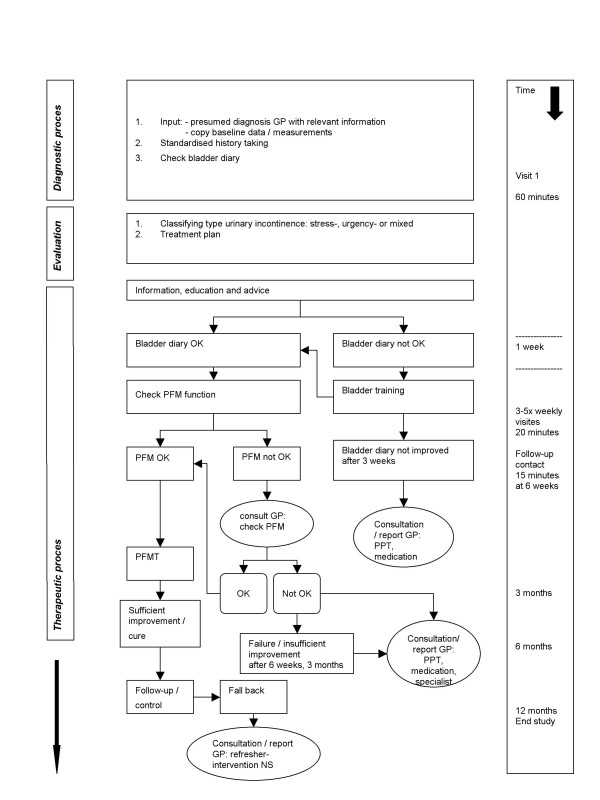
Background: Urinary incontinence affects approximately 5% (800.000) of the Dutch population. Guidelines recommend pelvic floor muscle/bladder training for most patients. Unfortunately, general practitioners use this training only incidentally, but prescribe incontinence pads. Over 50% of patients get such pads, costing 160 million euros each year. Due to ageing of the population a further increase of expenses is expected. Several national reports recommend to involve nurse specialists to support general practitioners and improve patient care. The main objective of our study is to investigate the effectiveness and cost-effectiveness of involving nurse specialists in primary care for urinary incontinence. This paper describes the study protocol.
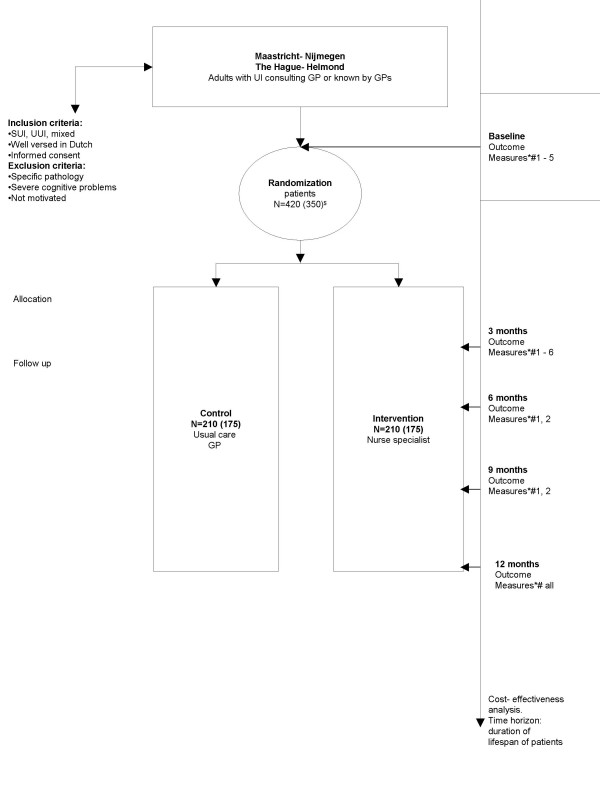
Methods/design: In a pragmatic prospective multi centre two-armed randomized controlled trial in the Netherlands the availability and involvement for the general practitioners of a nurse specialist will be compared with usual care. All consecutive patients consulting their general practitioner within 1 year for urinary incontinence and patients already diagnosed with urinary incontinence are eligible. Included patients will be followed for 12 months. Primary outcome is severity of urinary incontinence (measured with the International Consultation on Incontinence Questionnaire Short Form (ICIQ-UI SF)). Based on ICIQ-UI SF outcome data the number of patients needed to include is 350. For the economic evaluation quality of life and costs will be measured alongside the clinical trial. For the longer term extrapolation of the economic evaluation a Markov modelling approach will be used.
Discussion/conclusion: This is, to our knowledge, the first trial on care for patients with urinary incontinence in primary care that includes a full economic evaluation and cost-effectiveness modelling exercise from the societal perspective. If this intervention proves to be effective and cost-effective, implementation of this intervention is considered and anticipated.
Trial registration: Current Controlled Trials ISRCTN62722772.
Figures
References
-
- GIP/Health Insurance Board Total cost 2002-2006. 2007.
-
- Abrams P, Cardozo L, Khoury S, Wein A. Incontinence. 3rd International Consultation on Incontinence. 1&2. Monaco, Health Publication Ltd; 2005.
-
- Health Council of the Netherlands . Urinary Incontinence. The Hague, Health Council of the Netherlands; 2001.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
