

Treatment of hypovitaminosis D in infants and toddlers
- PMID: 18413426
- PMCID: PMC2729207
- DOI: 10.1210/jc.2007-2790
Treatment of hypovitaminosis D in infants and toddlers
Abstract
Context: Hypovitaminosis D appears to be on the rise in young children, with implications for skeletal and overall health.
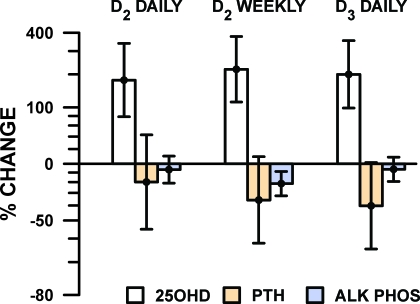
Objective: The objective of the study was to compare the safety and efficacy of vitamin D2 daily, vitamin D2 weekly, and vitamin D3 daily, combined with supplemental calcium, in raising serum 25-hydroxyvitamin D [25(OH)D] and lowering PTH concentrations.
Design: This was a 6-wk randomized controlled trial.
Setting: The study was conducted at an urban pediatric clinic in Boston.
Subjects: Forty otherwise healthy infants and toddlers with hypovitaminosis D [25(OH)D < 20 ng/ml] participated in the study.
Interventions: Participants were assigned to one of three regimens: 2,000 IU oral vitamin D2 daily, 50,000 IU vitamin D2 weekly, or 2,000 IU vitamin D3 daily. Each was also prescribed elemental calcium (50 mg/kg.d). Infants received treatment for 6 wk.
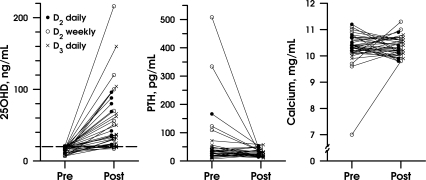
Main outcome measures: Before and after treatment, serum measurements of 25(OH)D, PTH, calcium, and alkaline phosphatase were taken.
Results: All treatments approximately tripled the 25(OH)D concentration. Preplanned comparisons were nonsignificant: daily vitamin D2 vs. weekly vitamin D2 (12% difference in effect, P = 0.66) and daily D2 vs. daily D3 (7%, P = 0.82). The mean serum calcium change was small and similar in the three groups. There was no significant difference in PTH suppression.
Conclusions: Short-term vitamin D2 2,000 IU daily, vitamin D2 50,000 IU weekly, or vitamin D3 2,000 IU daily yield equivalent outcomes in the treatment of hypovitaminosis D among young children. Therefore, pediatric providers can individualize the treatment regimen for a given patient to ensure compliance, given that no difference in efficacy or safety was noted among these three common treatment regimens.
Figures
Similar articles
-
Treatment of vitamin D insufficiency in children and adolescents with inflammatory bowel disease: a randomized clinical trial comparing three regimens.J Clin Endocrinol Metab. 2012 Jun;97(6):2134-42. doi: 10.1210/jc.2011-3182. Epub 2012 Mar 28. J Clin Endocrinol Metab. 2012. PMID: 22456619 Free PMC article. Clinical Trial.
-
Effects of High-Dose Vitamin D2 Versus D3 on Total and Free 25-Hydroxyvitamin D and Markers of Calcium Balance.J Clin Endocrinol Metab. 2016 Aug;101(8):3070-8. doi: 10.1210/jc.2016-1871. Epub 2016 May 18. J Clin Endocrinol Metab. 2016. PMID: 27192696 Free PMC article. Clinical Trial.
-
Heterogeneity in serum 25-hydroxy-vitamin D response to cholecalciferol in elderly women with secondary hyperparathyroidism and vitamin D deficiency.J Am Geriatr Soc. 2010 Aug;58(8):1489-95. doi: 10.1111/j.1532-5415.2010.02970.x. Epub 2010 Jul 14. J Am Geriatr Soc. 2010. PMID: 20646099 Clinical Trial.
-
Daily versus fortnightly oral vitamin D3 in treatment of symptomatic vitamin D deficiency in children aged 1-10 years: An open labelled randomized controlled trial.Clin Endocrinol (Oxf). 2024 Nov;101(5):491-498. doi: 10.1111/cen.15124. Epub 2024 Aug 13. Clin Endocrinol (Oxf). 2024. PMID: 39138889 Clinical Trial.
-
Pilot Study Evaluating Efficacy of 2 Regimens for Hypovitaminosis D Repletion in Pediatric Inflammatory Bowel Disease.J Pediatr Gastroenterol Nutr. 2016 Feb;62(2):252-8. doi: 10.1097/MPG.0000000000000915. J Pediatr Gastroenterol Nutr. 2016. PMID: 26196201 Free PMC article. Clinical Trial.
Cited by
-
Diagnosis and treatment of osteopenia.Rev Endocr Metab Disord. 2010 Dec;11(4):237-51. doi: 10.1007/s11154-010-9154-0. Rev Endocr Metab Disord. 2010. PMID: 21234807 Review.
-
National Cancer Institute, National Heart, Lung and Blood Institute/Pediatric Blood and Marrow Transplantation Consortium First International Consensus Conference on late effects after pediatric hematopoietic cell transplantation: the need for pediatric-specific long-term follow-up guidelines.Biol Blood Marrow Transplant. 2012 Mar;18(3):334-47. doi: 10.1016/j.bbmt.2012.01.003. Epub 2012 Jan 14. Biol Blood Marrow Transplant. 2012. PMID: 22248713 Free PMC article.
-
Vitamin D: deficiency, sufficiency and toxicity.Nutrients. 2013 Sep 13;5(9):3605-16. doi: 10.3390/nu5093605. Nutrients. 2013. PMID: 24067388 Free PMC article. Review.
-
Evaluation of ergocalciferol or cholecalciferol dosing, 1,600 IU daily or 50,000 IU monthly in older adults.J Clin Endocrinol Metab. 2011 Apr;96(4):981-8. doi: 10.1210/jc.2010-0015. Epub 2011 Feb 2. J Clin Endocrinol Metab. 2011. PMID: 21289249 Free PMC article. Clinical Trial.
-
DO IT Trial: vitamin D Outcomes and Interventions in Toddlers - a TARGet Kids! randomized controlled trial.BMC Pediatr. 2014 Feb 8;14:37. doi: 10.1186/1471-2431-14-37. BMC Pediatr. 2014. PMID: 24506910 Free PMC article. Clinical Trial.
References
-
- Ziegler EE, Hollis BW, Nelson SE, Jeter JM 2006 Vitamin D deficiency in breastfed infants in Iowa. Pediatrics 118:603-610 - PubMed
-
- Pettifor JM 2004 Nutritional rickets: deficiency of vitamin D, calcium, or both? Am J Clin Nutr 80:1725-1729 - PubMed
-
- Hollis BW, Wagner CL 2004 Assessment of dietary vitamin D requirements during pregnancy and lactation. Am J Clin Nutr 80(Suppl 6):1752S-1758S - PubMed
-
- Zittermann A 2003 Vitamin D in preventive medicine: are we ignoring the evidence? Br J Nutr 89:552-572 - PubMed
-
- Vasquez A, Manso G, Cannell J 2004 The clinical importance of vitamin D (cholecalciferol): a paradigm shift with implications for all healthcare providers. Altern Ther Health Med 10:28-36 - PubMed
