

Pathways to injury in chronic pancreatitis: decoding the role of the high-risk SPINK1 N34S haplotype using meta-analysis
- PMID: 18414673
- PMCID: PMC2289874
- DOI: 10.1371/journal.pone.0002003
Pathways to injury in chronic pancreatitis: decoding the role of the high-risk SPINK1 N34S haplotype using meta-analysis
Abstract
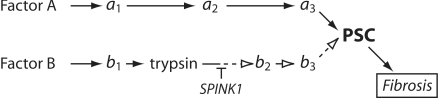
Background: The complex interactions between recurrent trypsin-mediated pancreatic injury, alcohol-associated pancreatic injury and SPINK1 polymorphisms in chronic pancreatitis (CP) are undefined. We hypothesize that CP occurs as a result of multiple pathological mechanisms (pathways) that are initiated by different metabolic or environmental factors (etiologies) and may be influenced differentially by downstream genetic risk factors. We tested this hypothesis by evaluating the differences in effect size of the high risk SPINK1 N34S haplotype on CP from multiple etiologies after combining clinical reports of SPINK1 N34S frequency using meta-analysis.
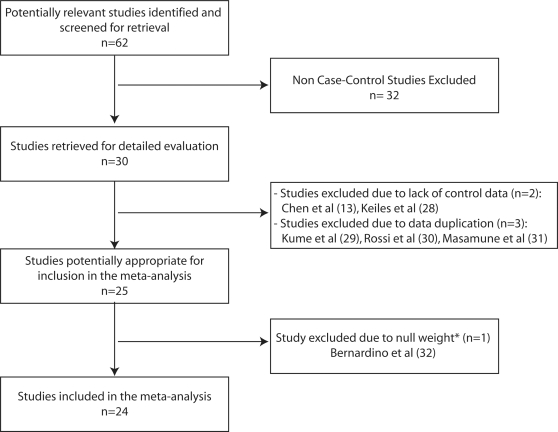
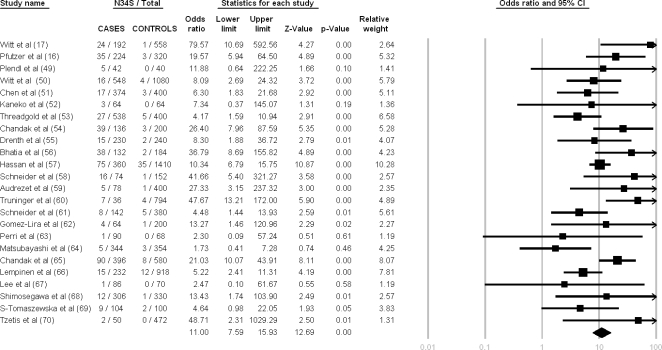
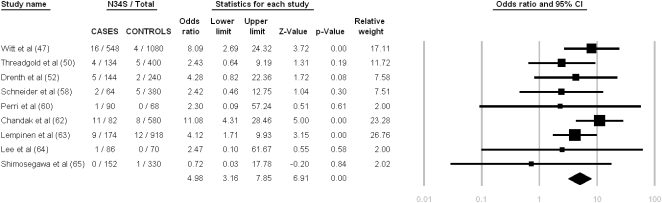
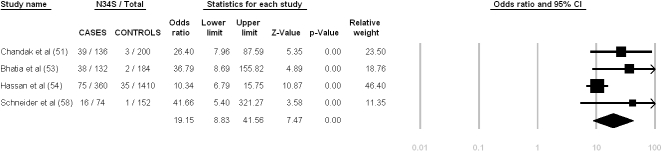
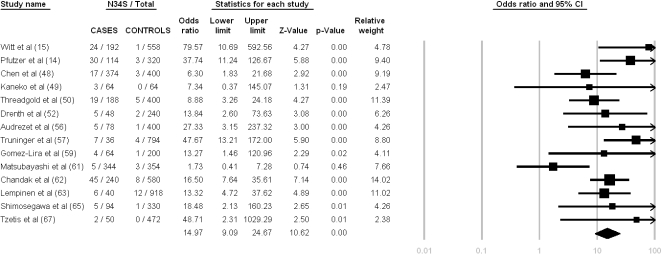
Methods and findings: The Pubmed and the Embase databases were reviewed. We studied 24 reports of SPINK1 N34S in CP (2,421 cases, 4,857 controls) using reported etiological factors as surrogates for pathways and multiple meta-analyses to determine the differential effects of SPINK1 N34S between alcoholic and non-alcoholic etiologies. Using estimates of between-study heterogeneity, we sub-classified our 24 studies into four specific clusters. We found that SPINK1 N34S is strongly associated with CP overall (OR 11.00; 95% CI: 7.59-15.93), but the effect of SPINK1 N34S in alcoholic CP (OR 4.98, 95% CI: 3.16-7.85) was significantly smaller than in idiopathic CP (OR 14.97, 95% C.I. = 9.09-24.67) or tropical CP (OR 19.15, 95% C.I. = 8.83-41.56). Studies analyzing familial CP showed very high heterogeneity suggestive of a complex etiology with an I(2) = 80.95%.
Conclusion: The small effect of SPINK1 N34S in alcoholic subjects suggests that CP is driven through a different pathway that is largely trypsin-independent. The results also suggest that large effect sizes of SPINK1 N34S in small candidate gene studies in CP may be related to a mixture of multiple etiologic pathways leading to the same clinical endpoint.
Conflict of interest statement
Figures
References
-
- Sarles H, Adler G, Dani R, Frey C, Gullo L, et al. The pancreatitis classification of Marseilles-Rome 1988. Scand J Gastroenterol. 1989;24:641–642. - PubMed
-
- Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med. 2006;354:2142–2150. - PubMed
-
- Etemad B, Whitcomb DC. Chronic pancreatitis: diagnosis, classification, and new genetic developments. Gastroenterology. 2001;120:682–707. - PubMed
-
- Steer ML, Waxman I, Freedman S. Chronic pancreatitis. N Engl J Med. 1995;332:1482–1490. - PubMed
-
- Warshaw AL, Banks PA, Fernandez-Del Castillo C. AGA technical review: treatment of pain in chronic pancreatitis. Gastroenterology. 1998;115:765–776. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
