

Does blood urea nitrogen level predict severity and high-risk endoscopic lesions in patients with nonvariceal upper gastrointestinal bleeding?
- PMID: 18414716
- PMCID: PMC2662899
- DOI: 10.1155/2008/207850
Does blood urea nitrogen level predict severity and high-risk endoscopic lesions in patients with nonvariceal upper gastrointestinal bleeding?
Abstract
Background: Nonvariceal upper gastrointestinal bleeding (UGIB) is a serious medical condition requiring prompt resuscitation and early endoscopic therapy in those with high-risk endoscopic lesions (HRLs). There are little or no data correlating sole blood urea nitrogen (BUN) level with the severity of nonvariceal UGIB or the presence of HRLs in the adult population.
Objectives: To determine if the BUN level on presentation correlates with parameters of severity of UGIB (need for blood transfusion or intensive care unit [ICU] admission) or to the subsequent finding of HRL, and in so doing identify patients who will require early endoscopic intervention.
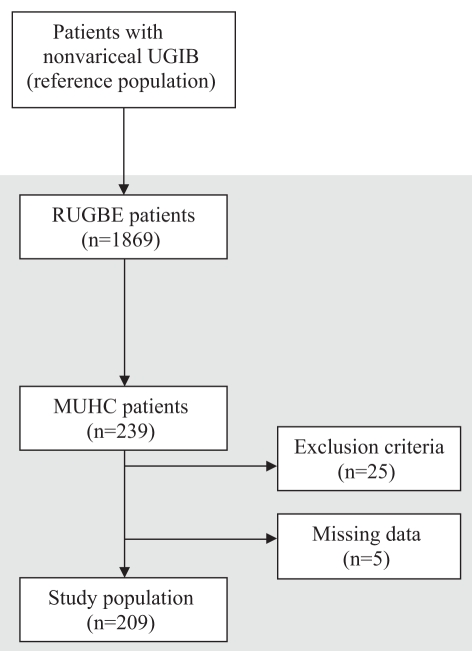
Methods: The Canadian Registry of patients with Upper Gastrointestinal Bleeding undergoing Endoscopy was used to identify patients enrolled from the McGill University Health Centre (Montreal, Quebec) who presented with or developed acute nonvariceal UGIB while admitted. All comparisons were performed using Student's t test or Wilcoxon's signed rank test, as appropriate. Logistic regression modelling using a stepwise method was performed to identify independent predictors of severe nonvariceal UGIB and HRL.
Results: Two hundred nine patients were enrolled in the study. The mean age was 67+/-18 years and 59.8% were male. The mean BUN level was 13.4+/-9.4 mmol/L. Univariate analysis demonstrated that the BUN level was a significant predictor of ICU admission (BUN 14.7+/-10.4 mmol/L versus 12.0+/-8.0 mmol/L, P=0.035). However, when adjusted for systolic blood pressure, BUN level became a weaker predictor of ICU admission, just failing to achieve statistical significance (OR 1.03, 95% CI 1.00 to 1.06; P=0.08). Univariate analysis also demonstrated that BUN level was not a statistically significant predictor of blood transfusion requirement (BUN 14.1+/-10.6 mmol/L versus 13.6+/-8.6 mmol/L, P=0.508), nor of HRL (BUN 14.2+/-10.7 mmol/L versus 12.9+/-8.6 mmol/L, P=0.605).
Conclusion: In patients with nonvariceal UGIB, the BUN level at initial presentation is a weak predictor of the severity of UGIB as defined by ICU admission, but is not helpful in identifying patients with a HRL.
HISTORIQUE :: L’hémorragie digestive haute (HDH) non variqueuse est une maladie grave qui requiert une réanimation rapide et un traitement endoscopique précoce chez les sujets atteints de lésions endoscopiques à risque élevé (LERÉ). Les données corrélant le taux d’azote uréique du sang (AUS) seul à la gravité de l'HDH non variqueuse ou à la présence de LERÉ sont peu nombreuses, voire inexistantes chez la population adulte.
OBJECTIFS :: Déterminer si le taux d’AUS au moment de la consultation est en corrélation avec les paramètres de gravité de l’HDH (dépendance transfusionnelle ou hospitalisation à l’unité des soins intensifs [USI]) ou avec la découverte subséquente des LERÉ permettant d’identifier des patients susceptibles de nécessiter une intervention endoscopique rapide.
MÉTHODES :: Les auteurs ont consulté le Registre canadien des patients atteints d’hémorragie digestive haute devant subir une endoscopie pour recenser les patients inscrits au Centre universitaire de santé McGill (Montréal, Québec) qui présentaient ou développaient une HDH aiguë au moment de leur admission. Toutes les comparaisons ont été réalisées à l’aide du test t de Student ou du test de Wilcoxon, selon le cas. Les différentes étapes du modèle de régression logistique ont été appliquées à l’identification des prédicteurs indépendants de l'HDH non variqueuse et des LERÉ graves.
RÉSULTATS :: Deux-cent-neuf patients ont été inscrits à l’étude, l’âge moyen était de 67 ± 18 ans et 59,8 % étaient de sexe masculin. Le taux moyen d’AUS était de 13,4 ± 9,4 mmol/L. L’analyse univariée a montré que le taux d’AUS était un prédicteur important de l’admission à l’unité des soins intensifs (USI) (AUS 14,7 ± 10,4 mmol/L, contre 12,0 ± 8,0 mmol/L, p = 0,035). Par contre, après ajustement pour tenir compte de la tension artérielle systolique, le taux d’AUS est devenu un prédicteur plus faible de l’hospitalisation à l’USI, à la limite de la portée statistique (RR 1,03, IC à 95 %, 1,00 à 1,06; p = 0,08). L’analyse univariée a aussi montré que le taux d’AUS n’était pas un prédicteur statistiquement significatif de la dépendance transfusionnelle (AUS 14,1 ± 10,6 mmol/L, contre 13,6 ± 8,6 mmol/L, p = 0,508) ni des LERÉ (AUS 14,2 ± 10,7 mmol/L, contre 12,9 ± 8,6 mmol/L, p = 0,605).
CONCLUSION :: Chez les patients qui présentent une HDH non variqueuse, le taux d’AUS au moment de la consultation est un faible prédicteur de la gravité de l’HDH définie par l’admission à l’USI, mais n’est pas utile au dépistage des LERÉ chez les patients atteints.
Figures
Similar articles
-
Association between an increase in blood urea nitrogen at 24 hours and worse outcomes in acute nonvariceal upper GI bleeding.Gastrointest Endosc. 2017 Dec;86(6):1022-1027.e1. doi: 10.1016/j.gie.2017.03.1533. Epub 2017 Apr 2. Gastrointest Endosc. 2017. PMID: 28377105
-
Three Simple Parameters on Admission to the Emergency Department are Predictors for Endoscopic Intervention in Patients with Suspected Nonvariceal Upper Gastrointestinal Bleeding.J Emerg Med. 2024 Feb;66(2):64-73. doi: 10.1016/j.jemermed.2023.08.016. Epub 2023 Sep 7. J Emerg Med. 2024. PMID: 38267298
-
Risk scoring systems to predict need for clinical intervention for patients with nonvariceal upper gastrointestinal tract bleeding.Am J Emerg Med. 2007 Sep;25(7):774-9. doi: 10.1016/j.ajem.2006.12.024. Am J Emerg Med. 2007. PMID: 17870480
-
Does this patient have a severe upper gastrointestinal bleed?JAMA. 2012 Mar 14;307(10):1072-9. doi: 10.1001/jama.2012.253. JAMA. 2012. PMID: 22416103 Review.
-
Acute, nonvariceal upper gastrointestinal bleeding.Curr Opin Crit Care. 2015 Apr;21(2):154-62. doi: 10.1097/MCC.0000000000000185. Curr Opin Crit Care. 2015. PMID: 25692808 Review.
Cited by
-
Blood Urea Nitrogen (BUN) is independently associated with mortality in critically ill patients admitted to ICU.PLoS One. 2018 Jan 25;13(1):e0191697. doi: 10.1371/journal.pone.0191697. eCollection 2018. PLoS One. 2018. PMID: 29370259 Free PMC article.
-
A quantitative exploration of gastrointestinal bleeding in intensive care unit patients.PLoS One. 2019 Feb 22;14(2):e0212040. doi: 10.1371/journal.pone.0212040. eCollection 2019. PLoS One. 2019. PMID: 30794554 Free PMC article.
-
Laboratory test variables useful for distinguishing upper from lower gastrointestinal bleeding.World J Gastroenterol. 2015 May 28;21(20):6246-51. doi: 10.3748/wjg.v21.i20.6246. World J Gastroenterol. 2015. PMID: 26034359 Free PMC article.
-
Patient characteristics with high or low blood urea nitrogen in upper gastrointestinal bleeding.World J Gastroenterol. 2015 Jun 28;21(24):7500-5. doi: 10.3748/wjg.v21.i24.7500. World J Gastroenterol. 2015. PMID: 26139996 Free PMC article.
-
Machine Learning Model for the Prediction of Hemorrhage in Intensive Care Units.Healthc Inform Res. 2022 Oct;28(4):364-375. doi: 10.4258/hir.2022.28.4.364. Epub 2022 Oct 31. Healthc Inform Res. 2022. PMID: 36380433 Free PMC article.
References
-
- Dulai GS, Gralnek IM, Oei TT, et al. Utilization of health care resources for low-risk patients with acute, nonvariceal upper GI hemorrhage: An historical cohort study. Gastrointest Endosc. 2002;55:321–7. - PubMed
-
- Silverstein FE, Gilbert DA, Tedesco FJ, Buenger NK. The national ASGE survey on upper gastrointestinal bleeding. I. Study design and baseline data. Gastrointest Endosc. 1981;27:73–9. - PubMed
-
- Longstreth GF. Epidemiology of hospitalization for acute upper gastrointestinal hemorrhage: A population-based study. Am J Gastroenterol. 1995;90:206–10. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical