

Review
doi: 10.1016/j.pbiomolbio.2008.02.024.
Epub 2008 Mar 5.
Cardiac resynchronization: insight from experimental and computational models
Affiliations
- PMID: 18417196
- PMCID: PMC2676869
- DOI: 10.1016/j.pbiomolbio.2008.02.024
Item in Clipboard
Review
Cardiac resynchronization: insight from experimental and computational models
Prog Biophys Mol Biol.
2008 Jun-Jul.
Abstract
Cardiac resynchronization therapy (CRT) is a promising therapy for heart failure patients with a conduction disturbance, such as left bundle branch block. The aim of CRT is to resynchronize contraction between and within ventricles. However, about 30% of patients do not respond to this therapy. Therefore, a better understanding is needed for the relation between electrical and mechanical activation. In this paper, we focus on to what extent animal experiments and mathematical models can help in order to understand the pathophysiology of asynchrony to further improve CRT.
Figures
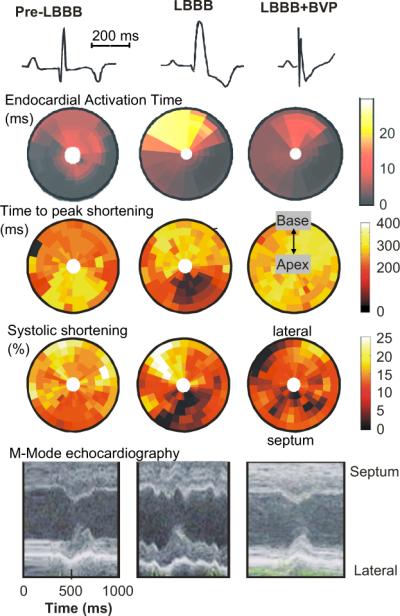
Electro-mechanics in the canine LBBB model. Examples of ECG (first row), endocardial electrical activation (2nd row), time to peak shortening (3rd row), percent systolic shortening (4th row) and endocardial wall motion (5th row), as observed before (left panels) and after inducing LBBB (middle panels) and during biventricular pacing (BVP) in the LBBB model (right panels). Timing of peak shortening is the time between the R wave and minimum circumferential strain. The % systolic shortening is the difference in circumferential strain between begin and end ejection. In the bulls-eye plots the lower half depicts the interventricular septum and the upper half the LV lateral wall; outer rings represent the base and inner rings the apex. Data are derived from (Vernooy et al., 2007). For each row the scale holds for each panel.
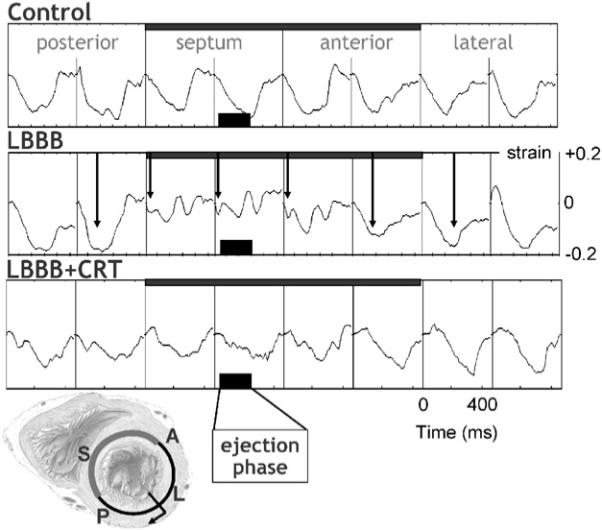
Typical example of myocardial circumferential strain tracings in eight regions along the circumference in a mid-basal short-axis LV slice. Strain was referenced to end-diastole. Arrows in the middle row indicate the time of peak shortening. Data are derived from Vernooy et al. (2007). Scales mentioned in one panel also hold for the other panels. The short axis section of the heart in the lower left corner illustrates the position of the eight regions of which the strains are derived from. P = posterior, S = septum, A = anterior.
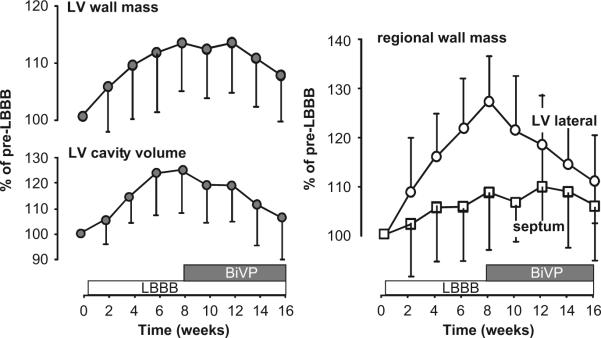
Time course of LV wall mass and cavity volume (left, global structural remodeling) and septal and LV free wall mass (regional structural remodeling, right) during 8 weeks of LBBB followed by 8 weeks of biventricular pacing in the canine heart. Data are derived from Vernooy et al. (2007). Mean values and SD are presented.
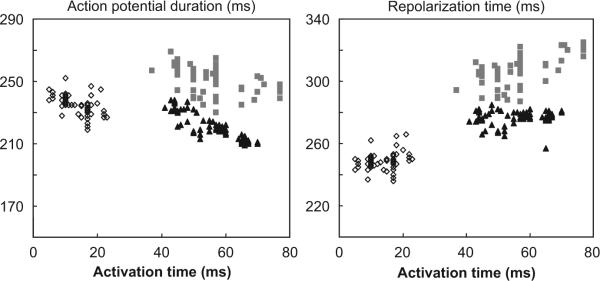
Action potential duration (left) and repolarization time (right) as a function of activation time of a canine heart during normal ventricular conduction (open diamonds), 1 h (grey squares) and 4 months after inducing LBBB (black triangles). Each data point represents measurement at one of 64 electrodes at the LV endocardium.
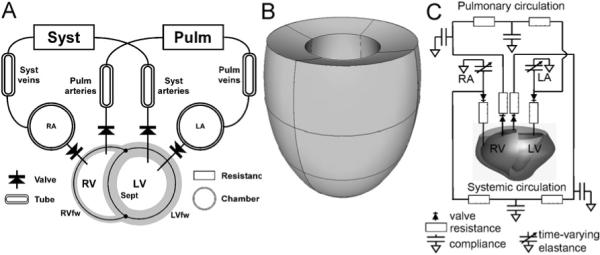
Three kinds of computational models. (A) The TriSeg/CircAdapt model. Three thick-walled spherical segments, i.e. the LV free wall segment (LVfw), the RV free wall segment (RVfw), and the septal wall segment (Sept) are coupled mechanically at the midwall junction, thus forming a left (LV) and a right (RV) ventricular cavity. Cardiac valves connect the atria to the ventricles (chamber module) and the ventricles to the systemic (Syst) and pulmonary (Pulm) circulations, containing tube and resistance modules. (B) Finite element model of the left ventricle, approximated by an ellipsoid (Kerckhoffs et al., 2003). (C) Hybrid finite element model of LV/RV and lumped parameter systems-model with a realistic geometry of a canine heart (Kerckhoffs et al., 2007b).
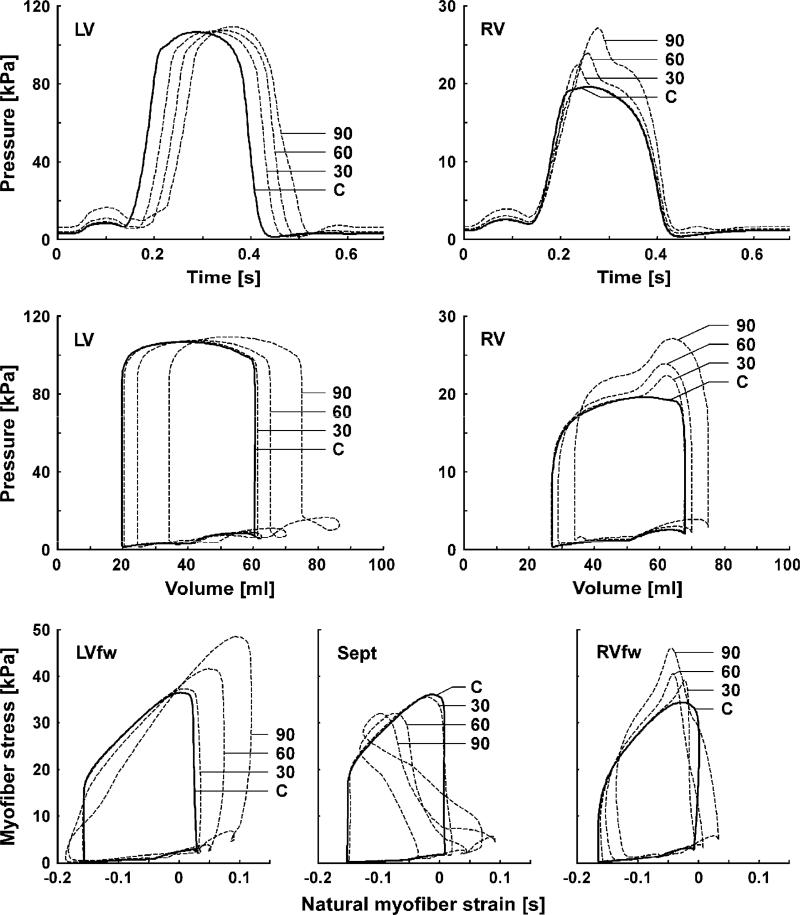
Left (LV) and right (RV) ventricular hemodynamics and myofiber mechanics as simulated with the TriSeg model in control (solid lines) and simulations with delayed activation of the LV (dashed lines). Top row: time courses of LV and RV pressures. Second row: LV and RV pressure–volume loops. Bottom row: predicted myofiber stress–strain loops of the LV free wall (LVfw), septal wall (Sept), and RV free wall (RVfw). Abbreviations C, 30, 60 and 90 indicate simulated results in control, and with delay of LV free wall activation by 30, 60 and 90 ms, respectively.
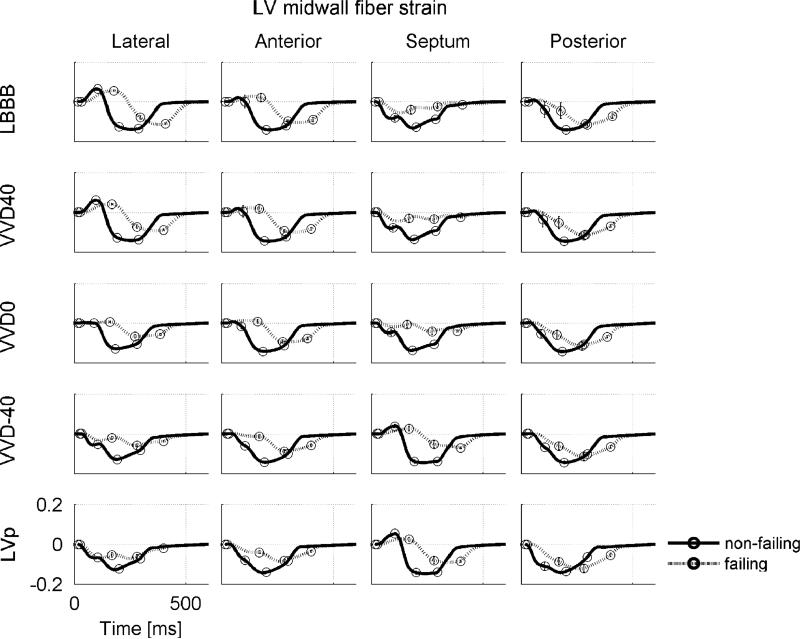
Fiber strain during a cardiac cycle in the LV midwall at the equator for all simulations. Cardiac phase transitions are indicated by circles, starting at end-diastole (which is also the state strain is referenced to). LBBB = left bundle branch block; VV-40, VV0 and VV40 = biventricular pacing with a RV–LV pacing interval of −40, 0 ms, and 40 respectively; LVp single site pacing at LV lateral wall. Scales mentioned in one panel also hold for the other panels.
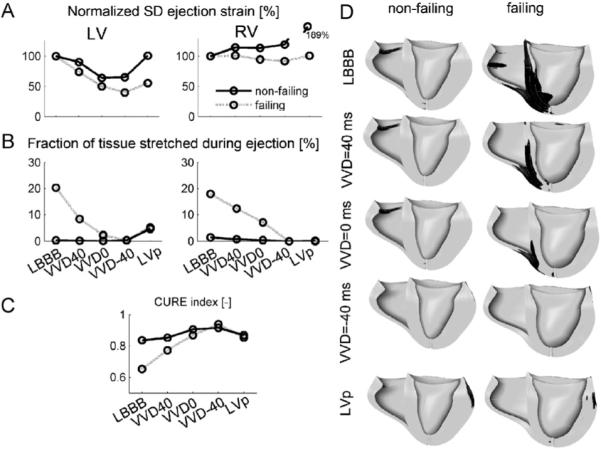
(A)–(C): Measures of regional mechanical dispersion in the hybrid model during various simulated pacing modes in the failing and non-failing heart. (A) Standard deviation of RV and LV ejection strain, normalized to LBBB, (B) fraction of tissue stretched during the ejection phase, (C) CURE index, and (D) regions in the ventricles that are stretched (black) during ejection. Abbreviations as in Fig. 7. Scales mentioned in one panel also hold for the other panels.
References
-
- Arts T, Delhaas T, Bovendeerd P, Verbeek X, Prinzen FW. Adaptation to mechanical load determines shape and properties of heart and circulation: the CircAdapt model. Am. J. Physiol. Heart Circ. Physiol. 2005;288:H1943–H1954. - PubMed
-
- Auricchio A, Stellbrink C, Block M, Sack S, Vogt J, Bakker P, Klein H, Kramer A, Ding J, Salo R, Tockman B, Pochet T, Spinelli J. Effect of pacing chamber and atrioventricular delay on acute systolic function of paced patients with congestive heart failure. The Pacing Therapies for Congestive Heart Failure Study Group. The Guidant Congestive Heart Failure Research Group. Circulation. 1999;99:2993–3001. - PubMed
-
- Baller D, Wolpers H-G, Zipfel J, Bretschneider H-J, Hellige G. Comparison of the effects of right atrial, right ventricular apex and atrioventricular sequential pacing on myocardial oxygen consumption and cardiac efficiency: a laboratory investigation. PACE. 1988;11:394–403. - PubMed
-
- Bax JJ, Abraham T, Barold SS, Breithardt OA, Fung JW, Garrigue S, Gorcsan J, 3rd, Hayes DL, Kass DA, Knuuti J, Leclercq C, Linde C, Mark DB, Monaghan MJ, Nihoyannopoulos P, Schalij MJ, Stellbrink C, Yu CM. Cardiac resynchronization therapy: part 1—issues before device implantation. J. Am. Coll. Cardiol. 2005;46:2153–2167. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
