

Carotid body tumors: objective criteria to predict the Shamblin group on MR imaging
- PMID: 18417602
- PMCID: PMC8119135
- DOI: 10.3174/ajnr.A1092
Carotid body tumors: objective criteria to predict the Shamblin group on MR imaging
Abstract
Background and purpose: MR imaging is an established method for diagnosis and surgical planning of carotid body tumors (CBTs). However no studies have elaborated preoperative objective criteria to predict the Shamblin (surgical) classification of CBTs, an important predictor of vascular morbidity. The purpose of this study was to establish criteria to accurately predict the Shamblin group on preoperative MR imaging for a uniform reporting system.
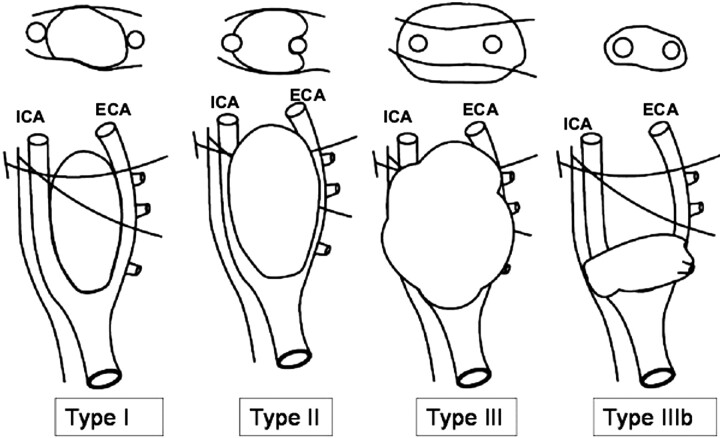
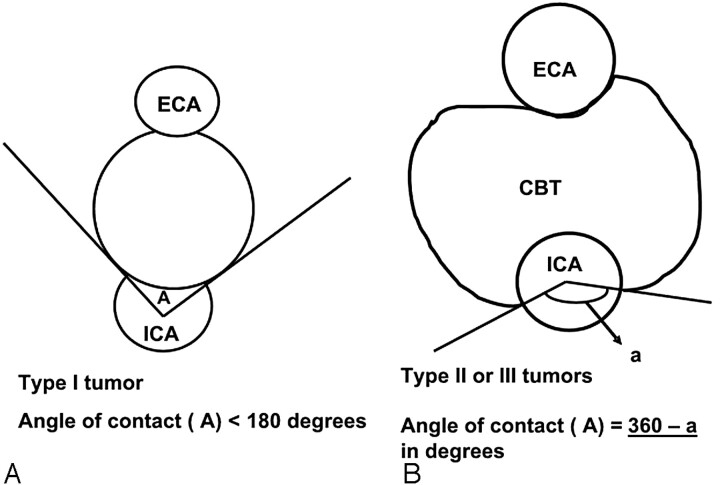
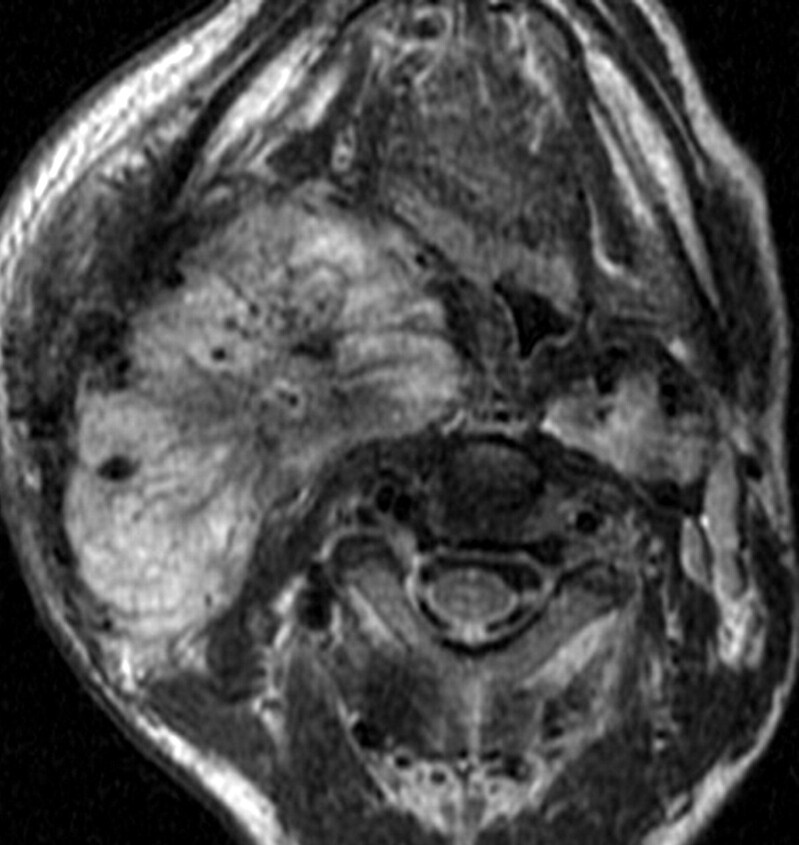
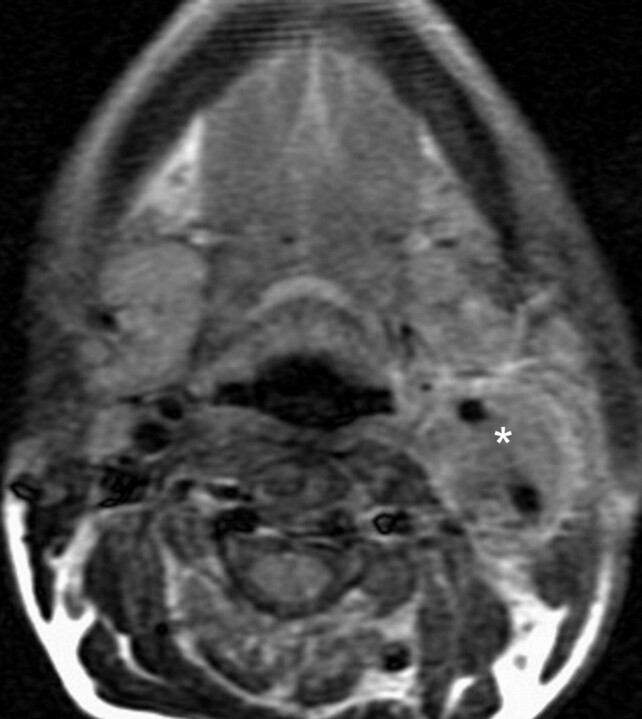
Materials and methods: MR images of 9 CBTs in 8 consecutive patients who underwent surgery between 2004 and 2007 were reviewed at a tertiary cancer hospital. The surgical records were blinded to the radiologists. A radiologic classification into 3 types (I, II, and III) based on the maximum degree of circumferential contact of the tumor with the internal carotid artery (ICA) was attempted and correlated with the Shamblin group in surgical records.
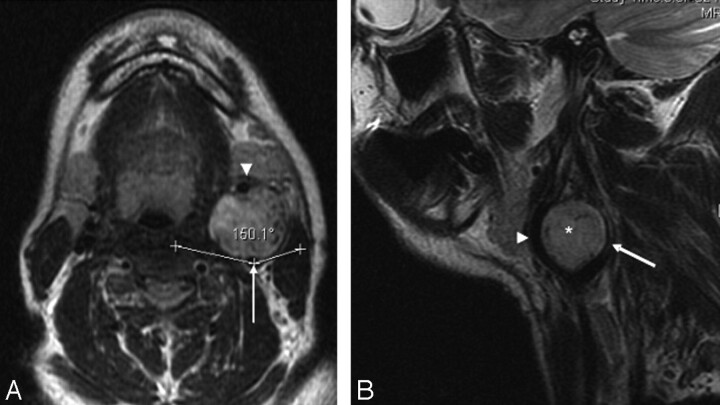
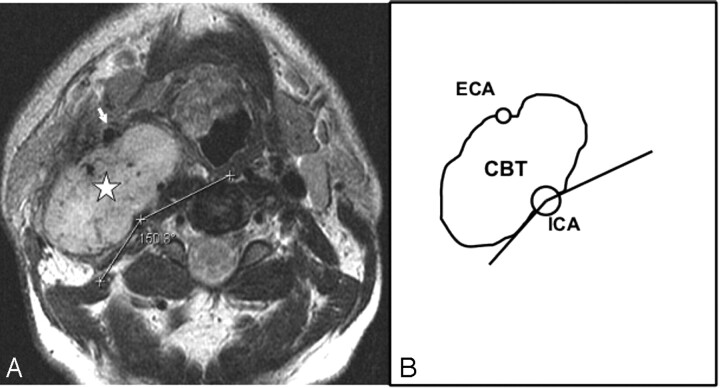
Results: There were 5 type III, 3 type II, and 1 type I tumors. The type I tumor had an ICA maximum circumference of contact less than or equal to 180 degrees , type II tumors had more than 180 degrees and less than 270 degrees , and type III tumors had a maximum circumference of contact of 270 degrees of more. MR imaging accurately predicted the Shamblin group in 8 (100%) of 8 operated tumors. Tumor size and Shamblin group did not have a uniformly predictable relation.
Conclusions: Shamblin group can be predicted preoperatively on MR imaging, and the maximum degree of circumferential contact of the CBT with the ICA on axial images is the criterion to predict the Shamblin group.
Figures
References
-
- Rao AB, Koeller KK, Adair CF. From the archives of the AFIP. Paragangliomas of the head and neck: radiologic-pathologic correlation Armed Forces Institute of Pathology Radiographics 1999;19:1605–32 - PubMed
-
- Shamblin WR, ReMine WH, Sheps SG, et al. Carotid body tumor (chemodectoma). Clinicopathologic analysis of ninety cases. Am J Surg 1971;122:732–39 - PubMed
-
- Knight TT Jr, Gonzalez JA, Rary JM, et al. Current concepts for the surgical management of carotid body tumor. Am J Surg 2006;191:104–10 - PubMed
-
- Luna-Ortiz K, Rascon-Ortiz M, Villavicencio-Valencia V, et al. Does Shamblin's classification predict postoperative morbidity in carotid body tumors? A proposal to modify Shamblin's classification. Eur Arch Otorhinolaryngol 2006;263:171–75 - PubMed
-
- van der Mey AGL, Jansen JC, van Baalen JM. Management of carotid body tumors. Otolaryngol Clin North Am 2001;34:907–24, vi - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous