

Surgical treatment of scoliosis: a review of techniques currently applied
- PMID: 18423027
- PMCID: PMC2346456
- DOI: 10.1186/1748-7161-3-6
Surgical treatment of scoliosis: a review of techniques currently applied
Abstract
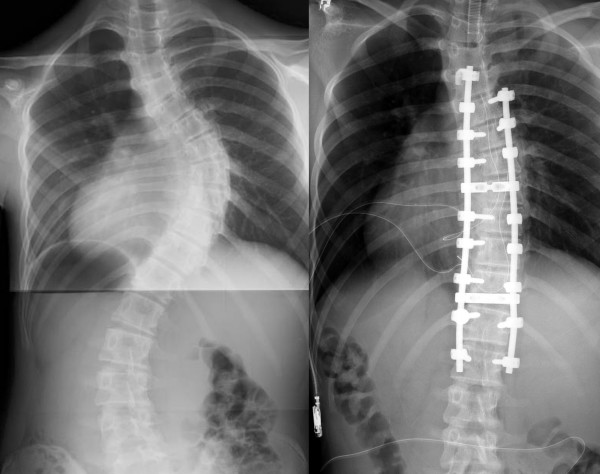
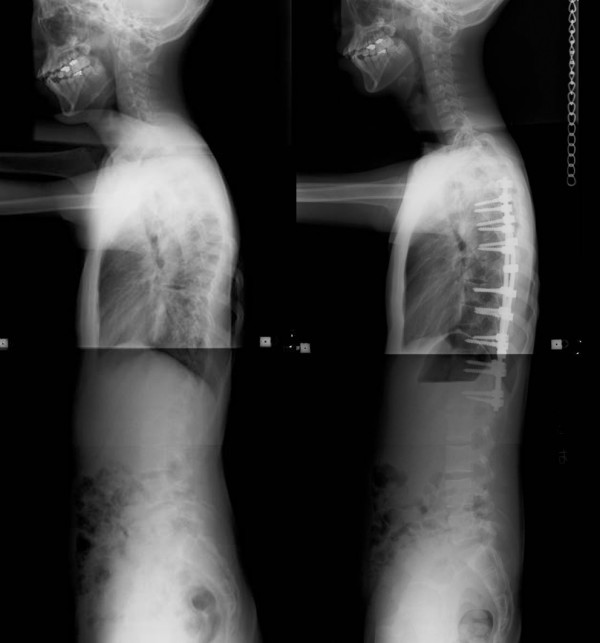
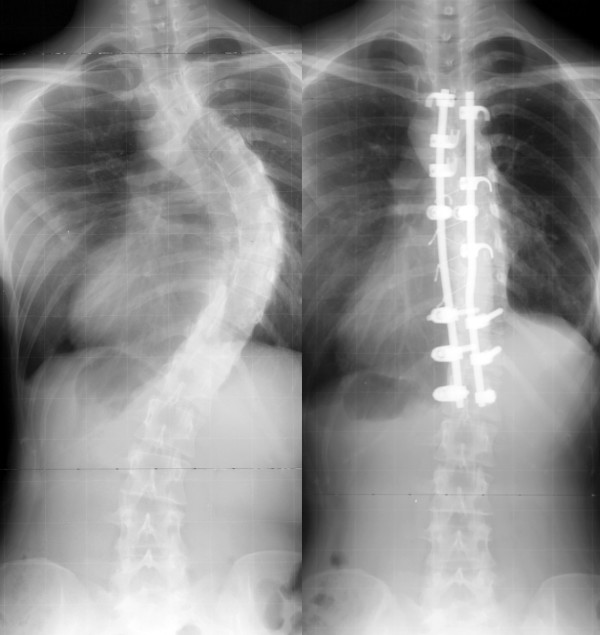
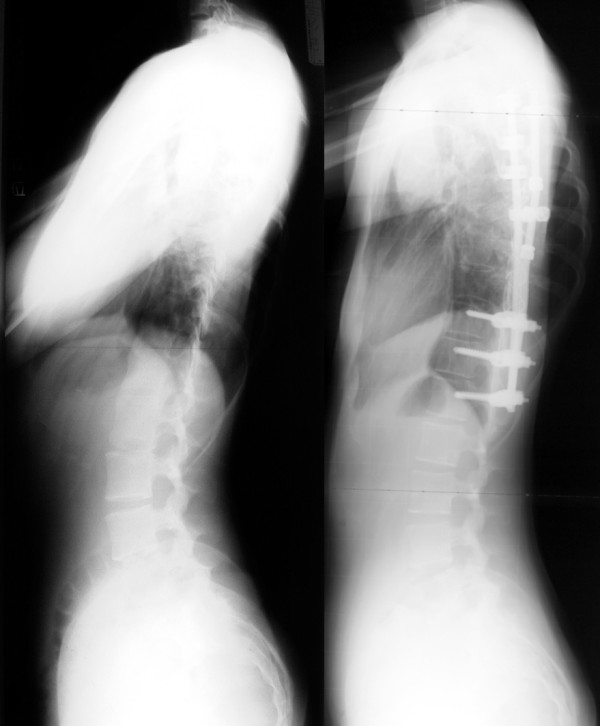
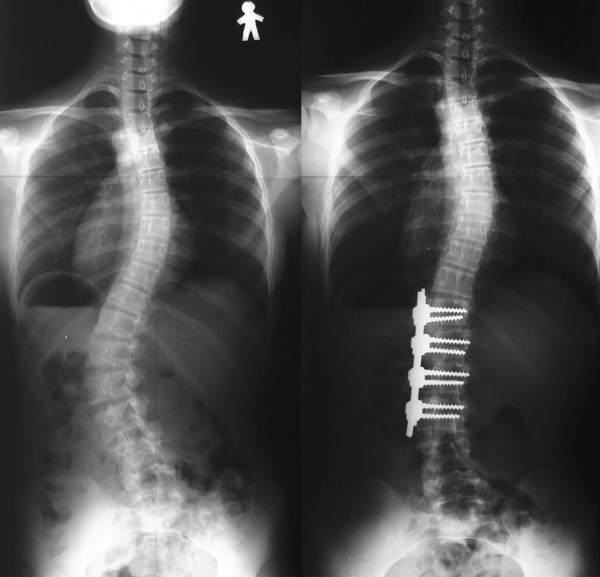
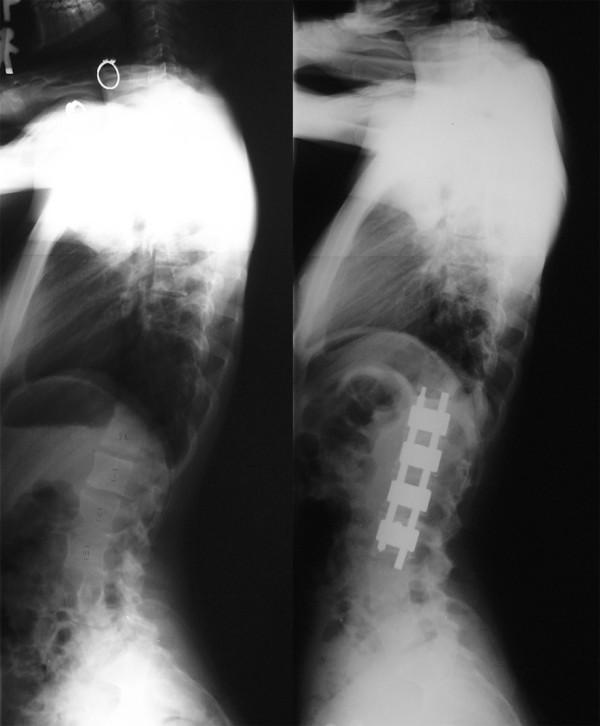
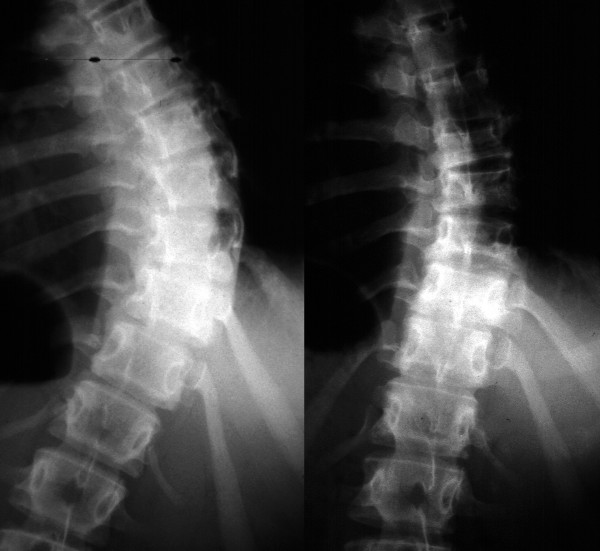
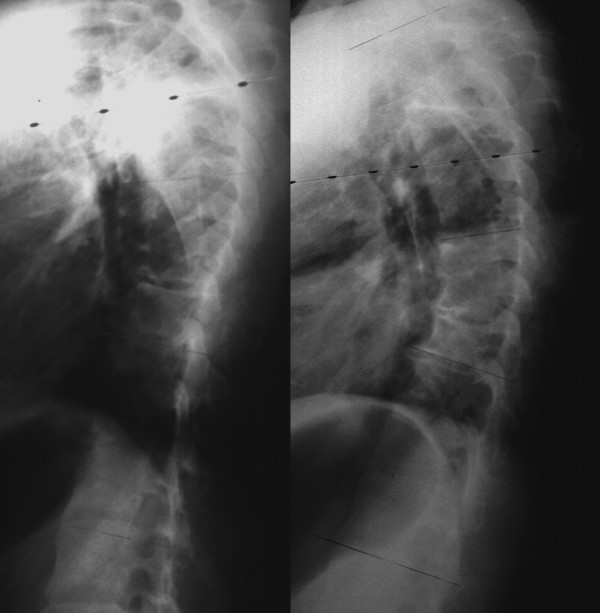
In this review, basic knowledge and recent innovation of surgical treatment for scoliosis will be described. Surgical treatment for scoliosis is indicated, in general, for the curve exceeding 45 or 50 degrees by the Cobb's method on the ground that:1) Curves larger than 50 degrees progress even after skeletal maturity.2) Curves of greater magnitude cause loss of pulmonary function, and much larger curves cause respiratory failure.3) Larger the curve progress, more difficult to treat with surgery.Posterior fusion with instrumentation has been a standard of the surgical treatment for scoliosis. In modern instrumentation systems, more anchors are used to connect the rod and the spine, resulting in better correction and less frequent implant failures. Segmental pedicle screw constructs or hybrid constructs using pedicle screws, hooks, and wires are the trend of today.Anterior instrumentation surgery had been a choice of treatment for the thoracolumbar and lumbar scoliosis because better correction can be obtained with shorter fusion levels. Recently, superiority of anterior surgery for the thoracolumbar and lumbar scoliosis has been lost. Initial enthusiasm for anterior instrumentation for the thoracic curve using video assisted thoracoscopic surgery technique has faded out.Various attempts are being made with use of fusionless surgery. To control growth, epiphysiodesis on the convex side of the deformity with or without instrumentation is a technique to provide gradual progressive correction and to arrest the deterioration of the curves. To avoid fusion for skeletally immature children with spinal cord injury or myelodysplasia, vertebral wedge ostetomies are performed for the treatment of progressive paralytic scoliosis. For right thoracic curve with idiopathic scoliosis, multiple vertebral wedge osteotomies without fusion are performed. To provide correction and maintain it during the growing years while allowing spinal growth for early onset scoliosis, technique of instrumentation without fusion or with limited fusion using dual rod instrumentation has been developed. To increase the volume of the thorax in thoracic insufficiency syndrome associated with fused ribs and congenital scoliosis, vertical expandable prosthetic titanium ribs has been developed.
Figures
References
-
- Weinstein SL, Ponseti IV. Curve progression in idiopathic scoliosis. J Bone Joint Surg Am. 1983;65:447–455. - PubMed
-
- Edgar M. The natural history of unfused scoliosis. Orthopedics. 1987;10:931–939. - PubMed
-
- Collis DK, Ponseti IV. Long-term follow-up of patients with idiopathic scoliosis not treated surgically. J Bone Joint Surg Am. 1969;51:425–445. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
