

Molecular profiles of progesterone receptor loss in human breast tumors
- PMID: 18425577
- PMCID: PMC2635926
- DOI: 10.1007/s10549-008-0017-2
Molecular profiles of progesterone receptor loss in human breast tumors
Abstract
Background: Patient prognosis and response to endocrine therapy in breast cancer correlate with protein expression of both estrogen receptor (ER) and progesterone receptor (PR), with poorer outcome in patients with ER+/PR- compared to ER+/PR+ tumors.
Methods: To better understand the underlying biology of ER+/PR- tumors, we examined RNA expression (n > 1000 tumors) and DNA copy number profiles from five previously published studies of human breast cancers with clinically assigned hormone receptor status (ER+/PR+, ER+/PR-, and ER-/PR-).
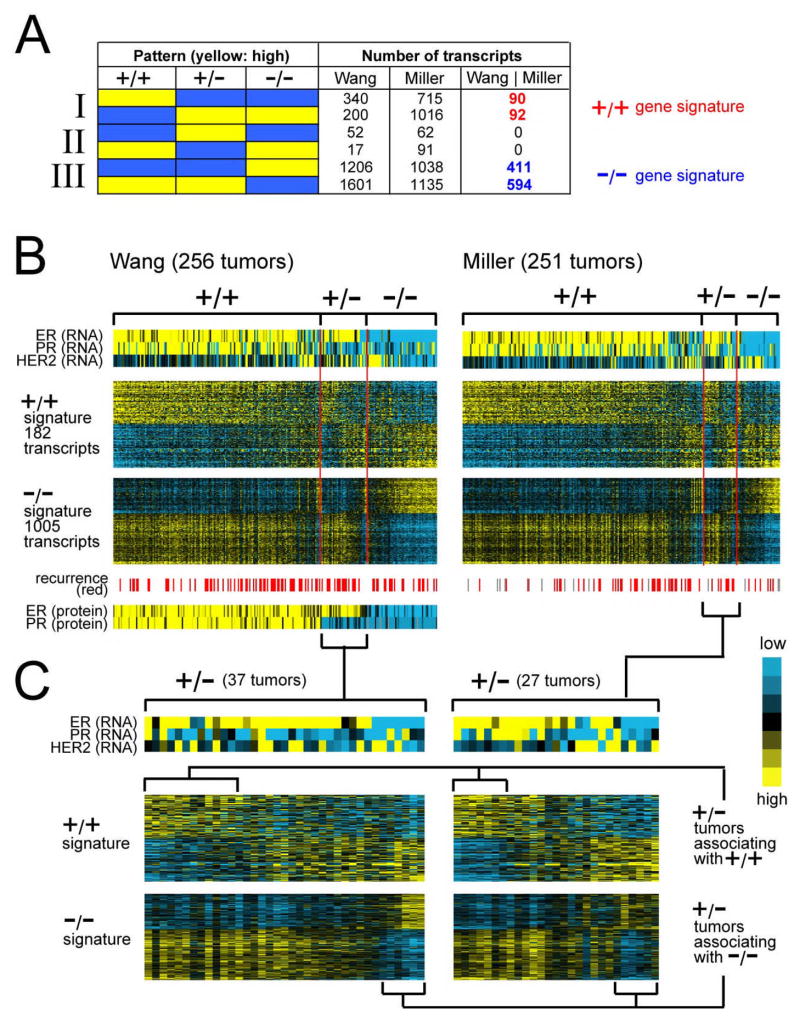
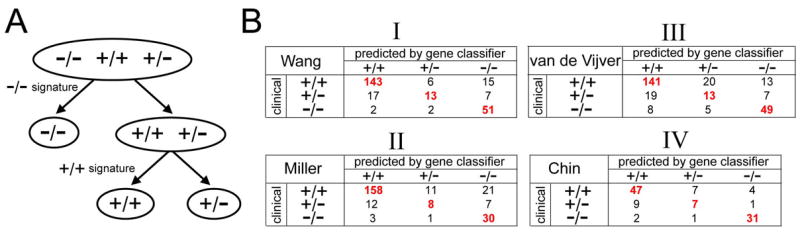
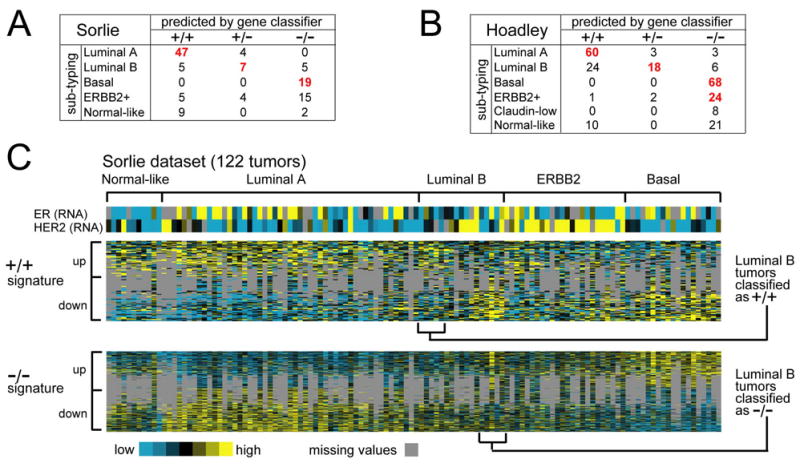
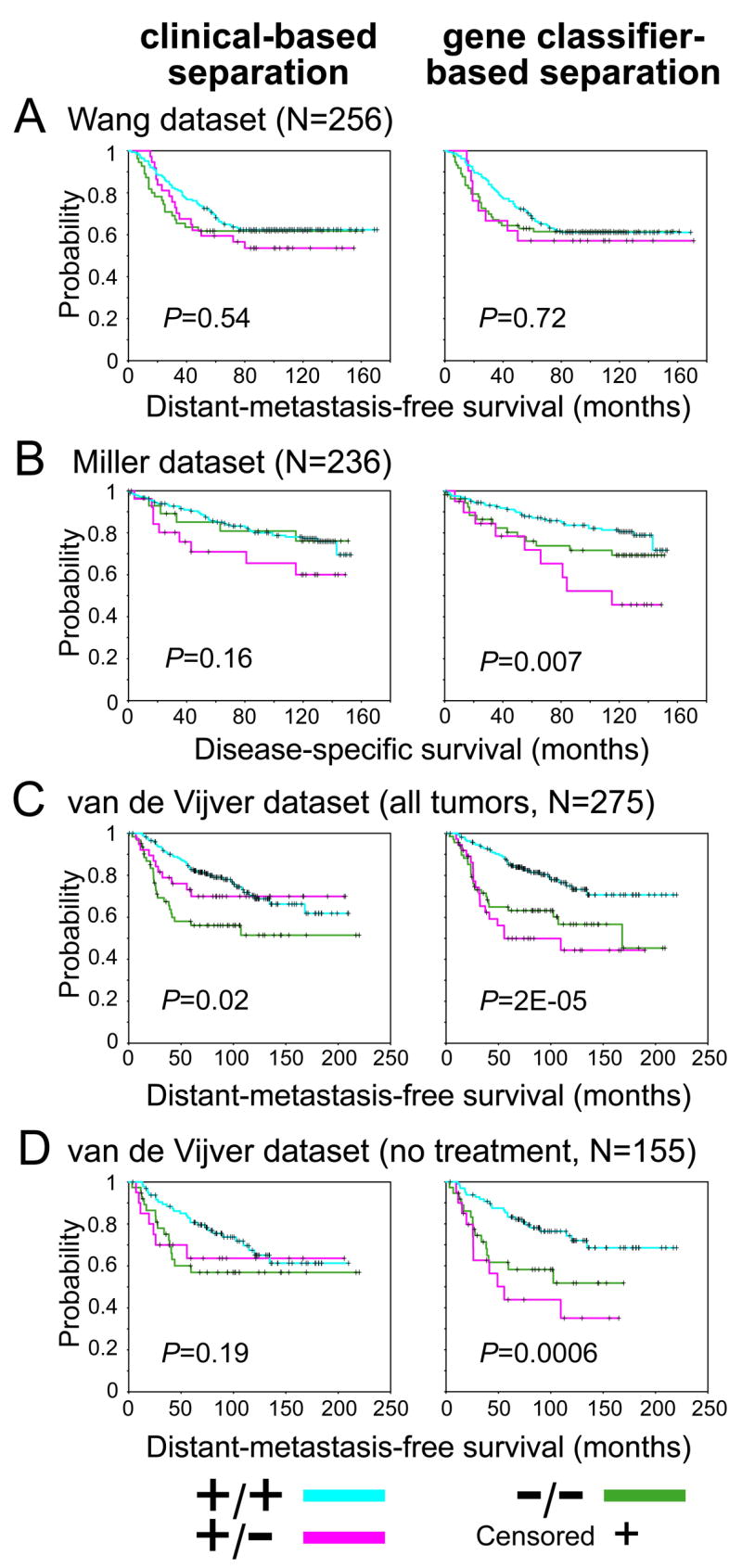
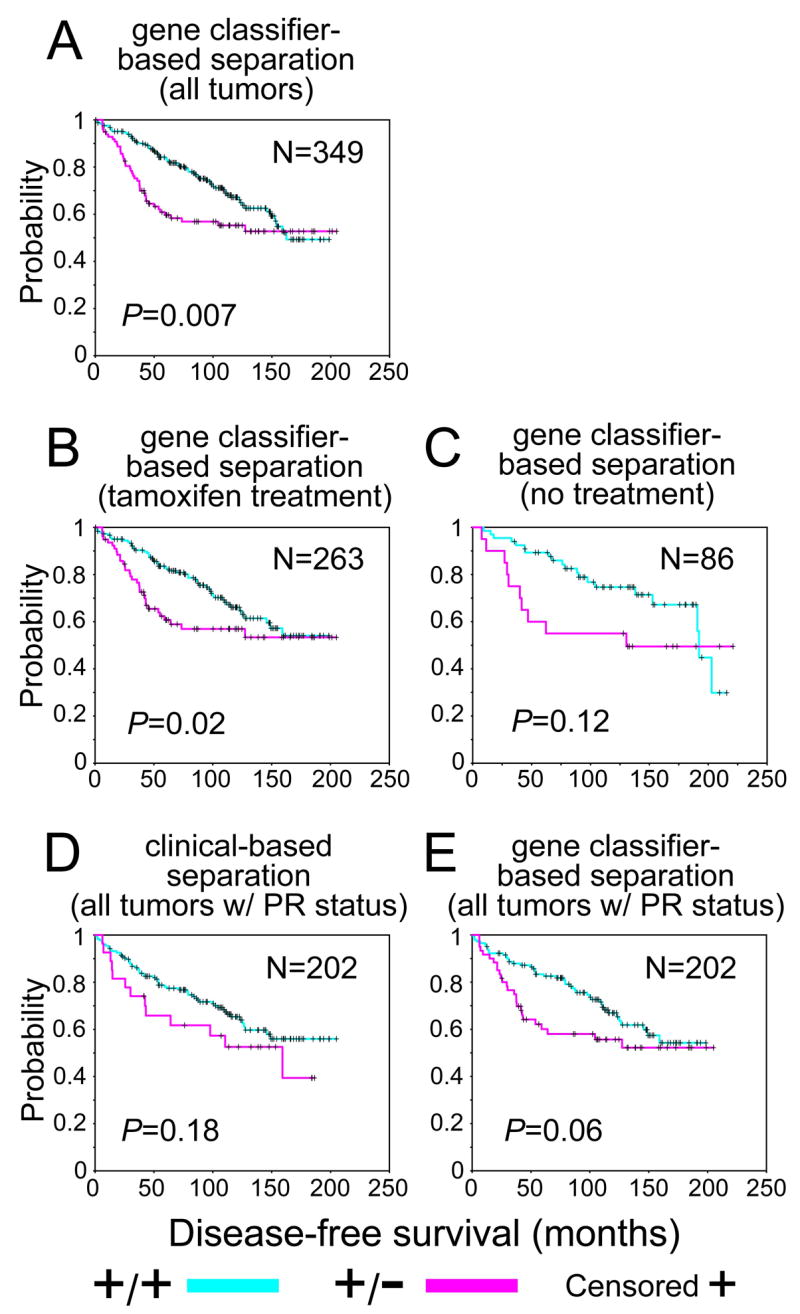
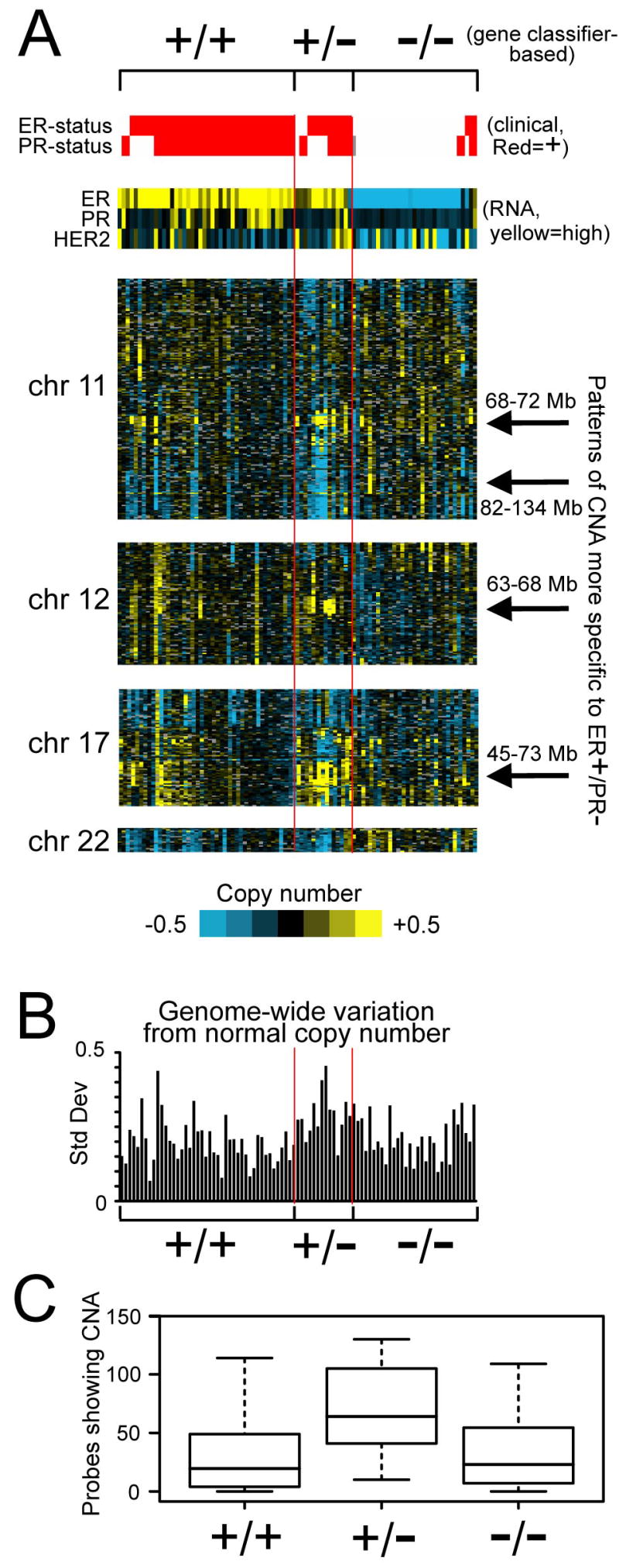
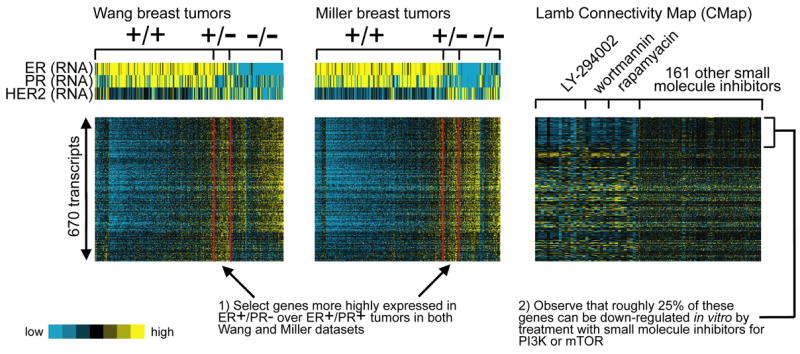
Results: We identified an expression "signature" of genes with either elevated or diminished RNA levels specifically in ER+/PR+ compared to ER-/PR- and ER+/PR- tumors. We similarly identified a gene signature specific to ER-/PR- tumors. ER+/PR- tumors, on the other hand, were a mixture of three different subtypes: tumors manifesting the ER+/PR+ signature, tumors manifesting the ER-/PR- signature, and tumors not associating with ER+/PR+ or ER-/PR- tumors (which we considered "true" ER+/PR-). In analyses of both tamoxifen-treated and untreated patients, ER+/PR- breast cancers defined by RNA profiling were associated with poor patient outcome, worse than those with pure ER+/PR+ patterns; these differences were not observed when using clinical assays to assign ER and PR status. ER+/PR- tumors also showed twice as many DNA copy number gains or losses compared to ER+/PR+ and ER-PR- tumors. Targets of transcriptional up-regulation by specific oncogenic pathways, including PI3 K/Akt/mTOR, were enriched in both ER+/PR- and ER-/PR- compared to ER+/PR+ tumors.
Conclusion: ER+/PR- tumors as defined by RNA profiling represent a distinct subset of breast cancer with aggressive features and poor outcome, despite being clinically ER+. Multigene assays derived from our gene signatures could conceivably provide an improved clinical assay for inferring PR status for prognostic and therapeutic purposes.
Figures
References
-
- Elledge RM, Fuqua SA. Estrogen and progesterone receptors. In: Harris J, Lippman ME, Morrow M, Osborne C, editors. Diseases of the Breast. Philadelphia: Lippincott, Williams and Wilkins; 2000. pp. 471–488.
-
- Cui X, Schiff R, Arpino G, Osborne CK, Lee AV. Biology of progesterone receptor loss in breast cancer and its implications for endocrine therapy. J Clin Oncol. 2005;23 (30):7721–7735. - PubMed
-
- Osborne C. Steroid hormone receptors in breast cancer management. Breast Cancer Res Treat. 1998;51(3):227–238. - PubMed
-
- Poole AJ, Li Y, Kim Y, Lin S-CJ, Lee W-H, Lee EYHP. Prevention of Brca1-mediated mammary tumorigenesis in mice by a progesterone antagonist. Science. 2006;314(5804):1467–1470. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
