

Resting magnetocardiography predicts 3-year mortality in patients presenting with acute chest pain without ST segment elevation
- PMID: 18426443
- PMCID: PMC6932191
- DOI: 10.1111/j.1542-474X.2008.00217.x
Resting magnetocardiography predicts 3-year mortality in patients presenting with acute chest pain without ST segment elevation
Abstract
Objective: Magnetocardiography (MCG) as a noninvasive, noncontact and risk-free diagnostic method predicts ischemic coronary artery disease (CAD) in patients with acute chest pain at admission with high accuracy. However, it remains unclear whether MCG findings can add prognostic information.
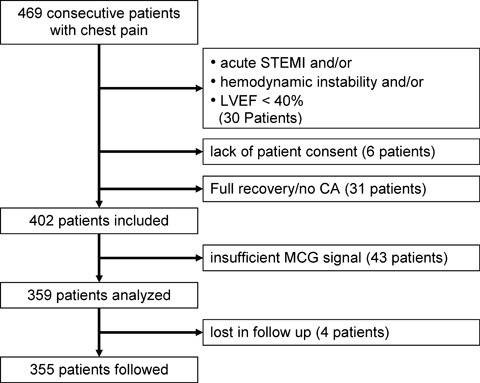
Method: A cohort of 402 consecutive patients presenting at the intensive care unit (ICU) with acute chest pain without ST segment elevation (NSTEMI) were included in a prospective registry. In order to prove the prognostic value of MCG a head-to-head comparison of the admission MCG, ECG, TnI, and ECHO tests was made.
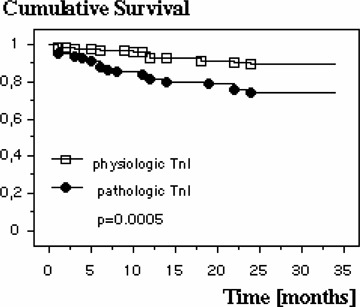
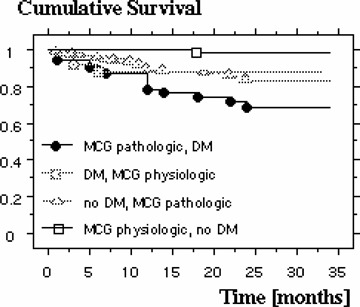
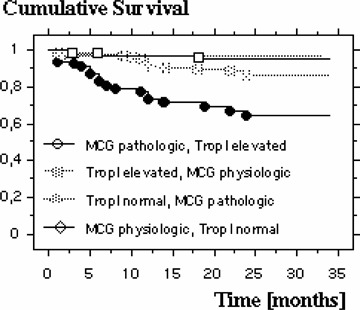
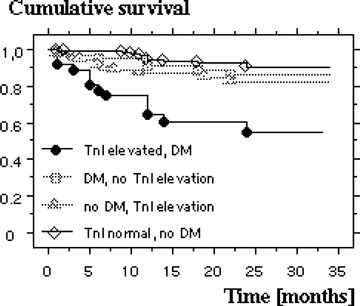
Results: In 43 patients (10.7%) the MCG could not be analyzed due to insufficient signal-to-noise ratio. Complete follow-up over a period of up to 3 years was obtained in 355 out of the 359 patients (98.9%). Age at admission was 67.2 +/- 10.3 years, 59.7% males. In the group of patients with an abnormal MCG at admission, 43 out of 249 patients (17.3%) died in the follow-up period, while in the group of patients with a normal MCG at admission only 4 out of 106 patients died (3.77%). The relative risk was 4.58 (95% confidence intervals: 1.68-12.42). A multivariate regression analysis revealed the highest mortality risk for patients with diabetes mellitus and an abnormal MCG at admission (RR = 18.0; 95% CI: 2.49-133.3).
Conclusion: Resting MCG at hospital admission predicts 3-year mortality in patients presenting with acute chest pain without ST segment elevation in the ECG. MCG seems to be valuable in identifying chest pain patients at highest risk.
Figures

References
-
- Giugliano RP, Braunwald E. The year in non‐ST‐segment elevation acute coronary syndromes. J Am Coll Cardiol 2005;46:906–919. - PubMed
-
- De Araujo GP, Ferreira J, Aguiar C, et al TIMI, PURSUIT, and GRACE risk scores: Sustained prognostic value and interaction with revascularization in NSTE‐ACS. Eur Heart J 2005;26:865–872. - PubMed
-
- Tang EW, Wong CK, Herbison P. Global Registry of Acute Coronary Events (GRACE) hospital discharge risk score accurately predicts long‐term mortality post acute coronary syndrome. Am Heart J 2007;153:29–35. - PubMed
-
- Theroux P, Fuster V. Acute coronary syndromes: Unstable angina and non‐Q‐wave myocardial infarction. Circulation 1998;97:1195–1206. - PubMed
-
- Ross R. Atherosclerosis–an inflammatory disease. N Engl J Med 1999;340:115–126. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
