

Baroreflex sensitivity: measurement and clinical implications
- PMID: 18426445
- PMCID: PMC6931942
- DOI: 10.1111/j.1542-474X.2008.00219.x
Baroreflex sensitivity: measurement and clinical implications
Abstract
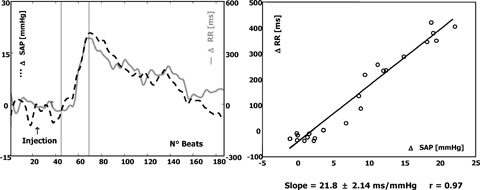
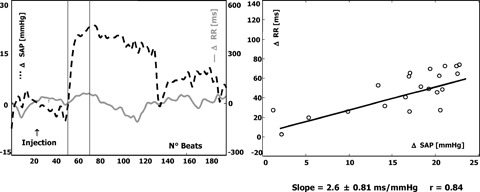
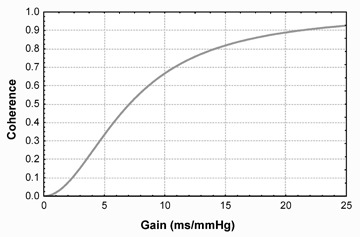
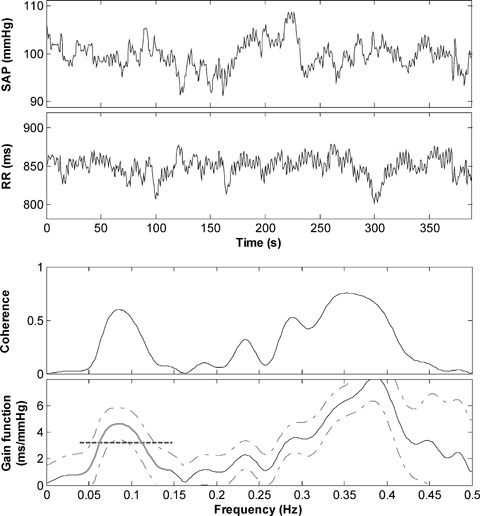
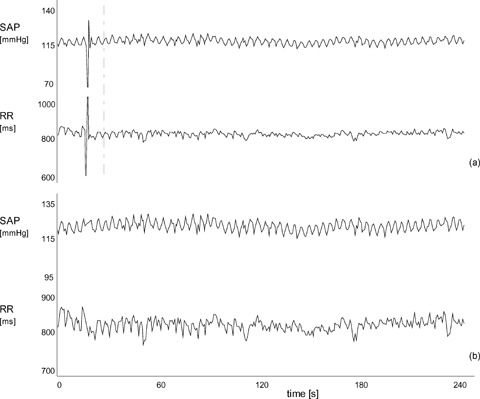
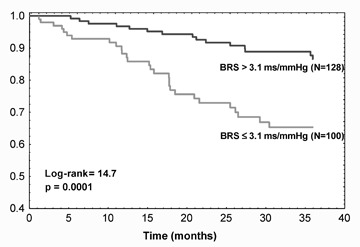
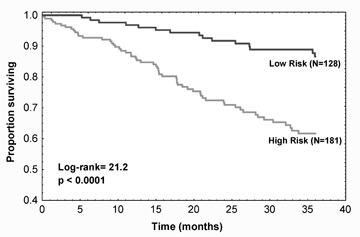
Alterations of the baroreceptor-heart rate reflex (baroreflex sensitivity, BRS) contribute to the reciprocal reduction of parasympathetic activity and increase of sympathetic activity that accompany the development and progression of cardiovascular diseases. Therefore, the measurement of the baroreflex is a source of valuable information in the clinical management of cardiac disease patients, particularly in risk stratification. This article briefly recalls the pathophysiological background of baroreflex control, and reviews the most relevant methods that have been developed so far for the measurement of BRS. They include three "classic" methods: (i) the use of vasoactive drugs, particularly the alpha-adrenoreceptor agonist phenylephrine, (ii) the Valsalva maneuver, which produces a natural challenge for the baroreceptors by voluntarily increasing intrathoracic and abdominal pressure through straining, and (iii) the neck chamber technique, which allows a selective activation/deactivation of carotid baroreceptors by application of a negative/positive pressure to the neck region. Two more recent methods based on the analysis of spontaneous oscillations of systolic arterial pressure and RR interval are also reviewed: (i) the sequence method, which analyzes the relationship between increasing/decreasing ramps of blood pressure and related increasing/decreasing changes in RR interval through linear regression, and (ii) spectral methods, which assess the relationship (in terms of gain) between specific oscillatory components of the two signals. The limitations of the coherence criterion for the computation of spectral BRS are discussed, and recent proposals for overcoming them are presented. Most relevant clinical applications of BRS measurement are finally reviewed with particular reference to patients with myocardial infarction and heart failure.
Figures
References
-
- Eckberg DL, Sleight P. Human Baroreflexes in Health and Disease. In: Eckberg DL, Sleight P, (eds): Oxford , Clarendon Press, 1992.
-
- Cowley AW Jr, Liard JF, Guyton AC. Role of baroreceptor reflex in daily control of arterial blood pressure and other variables in dogs. Circ Res 1973;32:564–576. - PubMed
-
- Kirchheim HR. Systemic arterial baroreceptor reflexes. Physiol Rev 1976;56:100–177. - PubMed
-
- Abboud FM, Thames MD. Interaction of cardiovascular reflexes in circulatory control In: Shepherd JT, Abboud FM. (eds): The Cardiovascular System. Bethesda, MD , American Physiological Society, 1983; pp. 675–754.
-
- Coleman TG. Arterial baroreflex control of heart rate in the conscious rat. Am J Physiol 1980;238:H515–H520. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
