

The OPALS Major Trauma Study: impact of advanced life-support on survival and morbidity
- PMID: 18427089
- PMCID: PMC2292763
- DOI: 10.1503/cmaj.071154
The OPALS Major Trauma Study: impact of advanced life-support on survival and morbidity
Abstract
Background: To date, the benefit of prehospital advanced life-support programs on trauma-related mortality and morbidity has not been established
Methods: The Ontario Prehospital Advanced Life Support (OPALS) Major Trauma Study was a before-after systemwide controlled clinical trial conducted in 17 cities. We enrolled adult patients who had experienced major trauma in a basic life-support phase and a subsequent advanced life-support phase (during which paramedics were able to perform endotracheal intubation and administer fluids and drugs intravenously). The primary outcome was survival to hospital discharge.
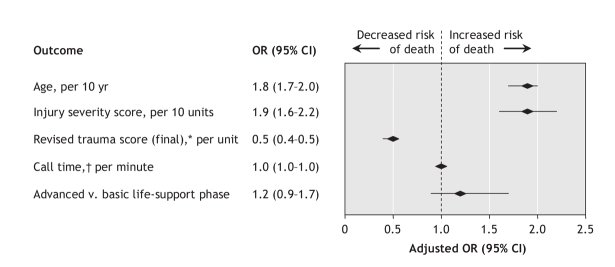
Results: Among the 2867 patients enrolled in the basic life-support (n = 1373) and advanced life-support (n = 1494) phases, characteristics were similar, including mean age (44.8 v. 47.5 years), frequency of blunt injury (92.0% v. 91.4%), median injury severity score (24 v. 22) and percentage of patients with Glasgow Coma Scale score less than 9 (27.2% v. 22.1%). Survival did not differ overall (81.1% among patients in the advanced life-support phase v. 81.8% among those in the basic life-support phase; p = 0.65). Among patients with Glasgow Coma Scale score less than 9, survival was lower among those in the advanced life-support phase (50.9% v. 60.0%; p = 0.02). The adjusted odds of death for the advanced life-support v. basic life-support phases were nonsignificant (1.2, 95% confidence interval 0.9-1.7; p = 0.16).
Interpretation: The OPALS Major Trauma Study showed that systemwide implementation of full advanced life-support programs did not decrease mortality or morbidity for major trauma patients. We also found that during the advanced life-support phase, mortality was greater among patients with Glasgow Coma Scale scores less than 9. We believe that emergency medical services should carefully re-evaluate the indications for and application of prehospital advanced life-support measures for patients who have experienced major trauma.
Figures
Comment in
-
Should invasive airway management be done in the field?CMAJ. 2008 Apr 22;178(9):1171-3. doi: 10.1503/cmaj.080234. CMAJ. 2008. PMID: 18427092 Free PMC article. No abstract available.
-
Prehospital and in-hospital advanced life-support.CMAJ. 2008 Jul 1;179(1):56. doi: 10.1503/cmaj.1080066. CMAJ. 2008. PMID: 18591535 Free PMC article. No abstract available.
References
-
- McCaig LF, Ly N. National Hospital Ambulatory Medical Care Survey: 2000 emergency department summary. Adv Data 2002;(326):1-30. - PubMed
-
- Maio RF, Garrison HG, Spaite DW, et al. Emergency Medical Services Outcomes Project I (EMSOP I): prioritizing conditions for outcomes research. Ann Emerg Med 1999;33:423-32. - PubMed
-
- Spaite DW, Criss EA, Valenzuela TD, et al. Prehospital advanced life support for major trauma: critical need for clinical trials. Ann Emerg Med 1998;32:480-9. - PubMed
-
- Carrico CJ, Holcomb JB, Chaudry IH; PULSE Trauma Work Group. Scientific priorities and strategic planning for resuscitation research and life saving therapy following traumatic injury: report of the PULSE Trauma Work Group. Post Resuscitative and Initial Utility of Life Saving Efforts. Shock 2002;17:165-8. - PubMed
-
- Lewis RJ. Prehospital care of the multiply injured patient: the challenge of figuring out what works. JAMA 2004;291:1382-4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical